
Abstract
Clustered Regularly Interspaced Short Palindromic Repeats (CRISPR) technology is a groundbreaking and dynamic molecular tool for DNA and RNA “surgery”. CRISPR/Cas9 is the most widely applied system in oncology research. It is a major advancement in genome manipulation due to its precision, efficiency, scalability and versatility compared to previous gene editing methods. It has shown great potential not only in the targeting of oncogenes or genes coding for immune checkpoint molecules, and in engineering T cells, but also in targeting epigenomic disturbances, which contribute to cancer development and progression. It has proven useful for detecting genetic mutations, enabling the large-scale screening of genes involved in tumor onset, progression and drug resistance, and in speeding up the development of highly targeted therapies tailored to the genetic and immunological profiles of the patient’s tumor. Furthermore, the recently discovered Cas12 and Cas13 systems have expanded Cas9-based editing applications, providing new opportunities in the diagnosis and treatment of cancer. In addition to traditional cis-cleavage, they exhibit trans-cleavage activity, which enables their use as sensitive and specific diagnostic tools. Diagnostic platforms like DETECTR, which employs the Cas12 enzyme, that cuts single-stranded DNA reporters, and SHERLOCK, which uses Cas12, or Cas13, that specifically target and cleave single-stranded RNA, can be exploited to speed up and advance oncological diagnostics. Overall, CRISPR platform has the great potential to improve molecular diagnostics and the functionality and safety of engineered cellular medicines. Here, we will emphasize the potentially transformative impact of CRISPR technology in the field of oncology compared to traditional treatments, diagnostic and prognostic approaches, and highlight the opportunities and challenges raised by using the newly introduced CRISPR-based systems for cancer diagnosis and therapy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The CRISPR family
The CRISPR (Clustered Regularly Interspaced Short Palindromic Repeats) family refers to a group of DNA sequences found in the genomes of bacteria and archaea. These sequences are part of an adaptive immune system that provides these microorganisms with resistance to foreign genetic elements, such as plasmids and phages [1]. The CRISPR components include: (a) CRISPR arrays represented by repeated DNA sequences interspaced with unique sequences called spacers, which are derived from viruses that have previously attacked the bacteria. Each spacer sequence corresponds to a fragment of viral DNA; (b) Cas (CRISPR-associated) proteins, a family of proteins that are essential for the CRISPR immune response, which has several members including the well-known Cas9 protein [2] and the most recently investigated Cas12 and Cas13, each with unique functions and properties [3, 4], as summarized in the Tables 1a and 1b.
Mechanistically, the CRISPR/Cas system operates in three stages: 1. Adaptation. When a bacterium is invaded by a virus, the CRISPR system captures a segment of the viral DNA and inserts it into the CRISPR array as a new spacer [5]. 2. Expression. The CRISPR array is transcribed into a long RNA molecule, which is then processed into shorter CRISPR RNAs (crRNAs) containing individual spacer sequences. 3. Interference, the process by which the CRISPR system inactivates the invading phage. The crRNAs guide the Cas proteins to the complementary viral DNA sequence, once there the Cas protein cleaves the DNA, neutralizing the viral threat [6]. The CRISPR/Cas systems are classified into two main classes and further into types and subtypes [7]. Class 1 involves multi-protein complexes for interference, e.g. Type I (Cas3), Type III (Cas10) and Type IV (Cas5 and Cas7). Class 2 uses a single, large Cas protein for interference, e.g. Type II (Cas9), Type V (Cas12) and Type VI (Cas13) [8].
A brief history of CRISPR-based systems
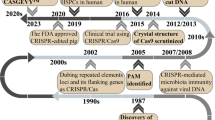
The CRISPR/Cas9 system is one of the most revolutionary scientific discoveries of recent decades, bringing gene editing to levels of precision and reliability that were unthinkable before [9]. The first CRISPR sequence was identified in 1987 by Ishino, who while analyzing the inhibitor of apoptosis (iap) gene in Escherichia coli, identified a series of 29-nucleotide repeats, interspersed with 32 to 33 nucleotide variable sequences, at the 3′-end of the gene [10]. In 1993, Mojica revealed the presence of similar DNA sequences in the halophilic archaeon Haloferax mediterranei [11] and, in 2000, Jansen coined the term CRISPR, highlighting the distinctive characteristic of this family of DNA sequences, which, unlike any other class of repetitive DNA, are interspaced by similarly sized non-repetitive DNA [12]. However, the biological function of CRISPR remained unknown until 2005, when Mojica demonstrated that these sequences were derived from viruses that had previously infected bacteria, suggesting that they functioned as an immune “memory” [13].
The breakthrough came in 2012, when Doudna and Charpentier demonstrated that the CRISPR/Cas9 system uses a dual-RNA structure, consisting of a crRNA and a trans-activating crRNA (tracrRNA), to guide the action of the Cas9 protein. This dual-RNA structure could be engineered as a single guide RNA (sgRNA) to direct the Cas9 enzyme towards specific regions of genomic DNA, allowing for extremely precise gene editing [14].
The first applications of CRISPR in cancer research was carried out in 2013 by Zhang [15] and Church [16], who demonstrated that, by using multiple gRNA sequences, the Cas9 enzyme can be directed to different sites in human and mouse cell lines, enabling multiple genome editing, ranging from small insertions and deletions (indels) to chromosomal deletions.
In 2015, Makarova defined two classes of CRISPR/Cas systems, with distinct evolutionary histories. The Class 1 system is characterized by multi-subunit effector complexes (type I, III, and IV), while the Class 2 system is associated with single-protein effector modules (types II, V, and VI) [17]. This classification provided a framework for understanding the different molecular architectures of CRISPR/Cas systems, stimulating scientists to search and identify previously unknown subtypes and novel proteins. Between 2015 and 2016, Abudayyeh identified two new CRISPR-based systems, in Francisella novicida, the Cas12 protein, a Class 2, Type V enzyme that could introduce targeted double-stranded breaks in DNA and, in Leptotrichia shahii, the Cas13 protein, a unique Class 2, Type VI CRISPR-associated enzyme, distinguished by its ability to target RNA rather than DNA [18, 19].
In 2016, with the emergence of immunotherapy, Marson explored the use of CRISPR/Cas9 to modify immune cells to enhance their ability to target cancer, and this approach was essential for the development of chimeric antigens receptor (CAR)-T cell therapies [20]. The CRISPR/Cas9-based editing method allowed the precise integration of the modified T cell receptor (TCR) in primary human T cells, without compromising their function, resulting in highly purified populations that stably expressed the new TCR [20]. In 2017, Patel used the CRISPR system, together with a machine-learning computational model, to identify genes essential for tumor progression in melanoma cell lines, such as collagen type XVII alpha 1 (COL17A1), twinfilin-1 (TWF1), microRNA 101-2 (Hsa-Mir-101-2) and ribosomal protein L23 (RPL23) [21]. These large-scale screenings allowed researchers to identify vulnerabilities in cancer cells that could be targeted for therapy. In 2020, Stadtmauer launched the first clinical trial testing the safety and feasibility of CRISPR/Cas9 editing in cancer patients [22]. The trial involved the CRISPR/Cas9-based deletion of the genes encoding TCRα, TCRβ and programmed cell death protein 1 (PD-1; PDCD1), in T cells derived from patients, followed by lentiviral transduction of a transgenic TCR specific for the cancer antigen New York oesophageal squamous cell carcinoma 1 (NY-ESO-1). The subsequent re-infusion of the engineered T cells resulted in durable engraftment, with editing in all genomic loci, and the modified cells persisted, in the circulation, for up to 9 months, indicating minimal immunogenicity [22].
Below, light will be shed on the current use and future perspectives offered by Cas9-, Cas12- and Cas13-based methods in experimental and clinical oncology.
Using the CRISPR/Cas9 system for cancer therapy and diagnosis
Cas9 (Class 2, Type II system) has a cis-cleavage function and causes double-stranded (ds)DNA breaks [23]. Cleavage activity for single-stranded (ss)DNA and ssRNA has also been reported in the presence of Protospacer Adjacent Motif (PAM)-presenting oligonucleotides (PAMmers) sequences designed to complement the target sequence (Fig. 1a) [24]. This property has been successfully used, coupled with real-time fluorescence analysis modalities, for the detection of specific nucleic acid targets [25]. Gene editing with the CRISPR/Cas9 system has shown great potential in both the treatment and diagnosis of cancer.
Applications of CRISPR/Cas9 for cancer treatment include gene editing and repair, immune enhancement strategies, and removal of anti-cancer drug resistance
-
1.
Gene editing and repair. CRISPR/Cas9 can precisely target and edit genes responsible for cancer initiation or progression, potentially deactivating oncogenes or activating tumor suppressor genes [26].
-
Targeting oncogenes. CRISPR/Cas9 can be used to specifically target, and knock-out, mutated or overexpressed oncogenes, such as MYC, KRAS, and EGFR, which drive tumor growth and progression [27, 28]. Interruption of the constitutively active tyrosine-kinase BCR/ABL1 Fusion Oncogene (FO) led to apoptosis and induced proliferative arrest of primary leukemic stem cells [29]. Disrupting two established FOs, involving either a transcription factor, EWSR1-FLI1 (EF), in Ewing sarcoma, or a tyrosine kinase, BCR-ABL1 (BA), in chronic myeloid leukemia, resulted in efficient cancer cell death and reduced tumor burden and mortality [30]. KRAS is the most frequently mutated oncogene in human cancers, thus representing an important therapeutic target. Knocking out mutated KRAS using CRISPR has been shown to inhibit colorectal cancer cell proliferation, both in vitro and in vivo [27].
CRISPR/Cas9 as proven to be effective in knocking out novel cancer drivers, such as interleukin(IL)-30 (IL27/p28) [31], which can both drive cancer stem cell expansion and exert immunosuppressive activity in the colorectal, prostate and breast cancer microenvironment [32,33,34]. Human IL-30 can be found as a membrane-anchored cytokine, expressed by cancer cells and by tumor-infiltrating macrophages and myeloid-derived suppressor cells (MDSCs) [33, 35] and plays a critical role in tumor onset and progression, by triggering a cascade of proinflammatory and oncogenic events, in association with the development of a robust vascular network [36, 37]. CRISPR/Cas9-mediated deletion of IL30 gene in stem or differentiated cancer cells has proven effective in hindering tumor growth and improve survival in colorectal and prostate cancer xenograft models [32, 33]. Moreover, intravenous administration of immunoliposomes that selectively convey Cas9gRNA-hIL30 complex for IL30 genome editing at the tumor, or metastatic sites, has shown to inhibit tumor growth and progression and improve survival without evident toxicity in xenograft and syngeneic PC models [38, 39].
-
Restoring tumor suppressor genes. CRISPR/Cas9 can be used to repair mutations or deletion in tumor suppressor genes, such as TP53, BRCA1, RB1 and PTEN, restoring their function and thereby halting disease progression [40, 41]. However, to make CRISPR/Cas9-mediated gene repair a viable therapeutic option, technical challenges, such as the low efficiency of Homology-Directed Repair (HDR), cell cycle dependence and the design of highly specific single guide RNAs (sgRNAs) to minimize off-target effects, urgently need to be addressed.
-
Epigenome editing. Epigenetic aberrations are known to cooperate with genetic alterations in driving the cancer phenotype [42]. Targeting the cancer epigenome with CRISPR technology is currently being developed for cancer therapy [43, 44]. By fusing a catalytically dead form of Cas9, namely nuclease-deficient Cas9 (dCas9), with epigenetic modifiers, such as Dnmt3a (a DNA methylation enzyme) or Tet1 (a DNA demethylation enzyme), gene expression can be modulated without changing the DNA sequence [45]. These tools can add or remove epigenetic marks and reverse cancer-associated epigenetic changes [45]. Epigenetic therapies have proven to sensitize patients to the reversal of immune tolerance and to improve the efficacy of immune checkpoint therapies [46] in metastatic non-small cell lung cancer (NSCLC) [47], however a perspective use of CRISPR/dCas for epigenetic editing as an anti-cancer strategy requires in depth investigation and testing in combined therapies, as cancer results from a combination of genetic and epigenetic alterations [48].
-
2.
Immunotherapy enhancement. CRISPR/Cas9 can be used to engineer T cells to express chimeric antigen receptors [49, 50], to delete inhibitory immune checkpoint expression in T and NK cells [51], and to identify and delete genes involved in drug resistance and enhance treatment efficacy [52,53,54].
-
Engineering T cells. CRISPR/Cas9 can be used to edit the genome of T lymphocytes to enhance their ability to recognize and kill cancer cells. This includes engineering T cells to express Chimeric Antigen Receptors (CAR-T), that can specifically target cancer cells. Bispecific T cells are generated by introducing genes that encode TCRs and CARs of the desired specificity and affinity for tumors [49]. CRISPR was successfully used to engineer T cells to express CARs targeting CD19 in patients with B-cell lymphoma leading to durable remissions in a significant proportion of treated patients [55]. CRISPR has been useful in the development of non-autologous CAR-T cells that could be used in any patient without the need for HLA matching, thereby reducing costs and making CAR T-cell therapy accessible to patients lacking sufficient healthy T lymphocytes required for treatment [56].
-
Deleting immune checkpoints. CRISPR/Cas9 can knock-out genes coding for immune checkpoint proteins, such as PDCD1 gene, which encodes for PD-1, in primary T lymphocytes [57], or in NK cells [58], and maximize PD-1/Programmed cell Death Ligand 1 (PD-L1) deletion at the genomic level, thereby saving the function of lymphocytes, or NK cells, against tumors. CRISPR/Cas9-mediated disruption of immune checkpoint signaling, such as PD-1, enhances the therapeutic efficacy of CAR-T cells in the immunosuppressive tumor microenvironment [55].
-
3.
Drug resistance reversal. The development of therapy resistance is a major obstacle to cancer treatment [59]. Cancer cells resist anticancer drugs by a variety of mechanisms, such as enhancing drugs efflux, enhancing DNA repair, enhancing stemness, inhibiting apoptosis, and altering drug target [60]. Mutations of genes implicated in specific signaling pathways may underlie these events and lead to drug resistance. CRISPR technology allows the identification of genes involved in therapy resistance and their editing to sensitize cancer cells to therapy.
-
Identifying genes involved in resistance to antitumor therapy. Genome-wide CRISPR knock-out screens technique is used to identify genes involved in drug resistance. CRISPR screens proved that mutations of Polybromo-1 (PBRM1) gene attenuate the effects of EGFR inhibitors in lung cancer by enhancing the continuity of AKT signaling [61]. Gene silencing using the CRISPR/Cas9sgRNA system has revealed that loss of Shugoshin 1 (SGOL1), that plays a crucial role in cell mitosis, may cause resistance to sorafenib in hepatocellular carcinoma [62]. CRISPR/Cas9 screens also defined the importance of the MSH2 gene and mismatch repair in cisplatin resistance in bladder cancer [63] and the role of ABCB1 gene (also named multidrug resistance1, MDR1, which encodes a transmembrane glycoprotein transporting multiple types of chemotherapeutic drugs out of cells) in breast cancer resistance to doxorubicin [64, 65]. The key role of MSH2, Chloride Channel Accessory 2 (CLCA2), and Patched 2 (PTCH2), in the resistance of glioblastoma cells to temozolomide was elucidated using genome-wide CRISPR/Cas9 screen technology [66].
Poly(ADP-ribose) polymerase (PARP) inhibitors (PARPis) selectively induce synthetic lethality in cancer cells harboring mutations in the BRCA1/2 genes [67]. Genome-wide CRISPR/Cas9 knock-out screens in BRCA1/2-proficient prostate cancer (PC) cells identified genes whose loss has a profound impact on PARPis response and find that loss of Checkpoint Kinase 2 (CHEK2), which is involved in the DNA damage repair response, confers PARPis resistance in PC cells with functional p53 [68], and that deletion of Ribonuclease H2 Subunit B (RNASEH2B), which play a role in DNA replication, confers PC cell sensitivity to PARPis [69].
-
Sensitizing cancer cells to antitumor therapy. CRISPR/Cas9 can be used to edit genes that contribute to drug resistance, making the cancer cells more susceptible to existing treatments [70]. CRISPR/Cas9 mediated knocking out of glutathione S-Transferase Omega 1 (GSTO1) in colorectal cancer cells enhances the cytotoxicity of chemotherapeutics, including cisplatin and oxaliplatin [71]. CRISPR/Cas9-mediated knock-out of ABCB1/MDR1 gene significantly enhances the chemosensitivity of colorectal cancer cells to doxorubicin (DOX) [65, 72]. Targeting MDR1 using CRISPR/Cas9 system in DOX-resistant breast cancer cells increases drug uptake and intracellular accumulation compared with untreated cells resulting in improved DOX cytotoxicity [64].
Besides being an immune checkpoint molecule and preventing anti-tumor T cell response, PD-L1 (B7-H1, CD274) has a cancer cell-intrinsic pro-survival function and may contribute to cancer chemoresistance. Activation of multiple signaling pathways promotes multi drug resistance in breast cancer. Notably, activating PhosphatidylInositol 3-Kinase (PI3K)/AKT and mitogen-activated protein kinase (MAPK)/ERK pathways can increase the expression of ABCB1 and enhance DOX resistance [73]. PD-L1 knock-out by CRISPR/Cas9 has proven effective in making triple negative breast cancer cells susceptible to chemotherapy through a reduced activation of p38 MAPK signalling pathway, that is dependent on the association of DNA-PKcs and B7-H1 followed by a downregulation of Bcl-2 [74].
Applications of CRISPR/Cas9 for molecular diagnostics and prognosis of tumors
CRISPR/Cas9 can be used for early detection and screening of cancer-associated mutations, after capturing circulating tumor (ct) DNA or circulating tumor cells (CTC) in blood samples, obtained through liquid biopsies [75]. This non-invasive approach allows for early cancer detection and monitoring of tumor dynamics over time providing insights into disease progression and potential resistance to therapy. Integrating biosensors, that convert a biological response into an electrical signal, with CRISPR/Cas technology, can enhance the detection of specific cancer-related genetic sequences and identify mutations in oncogenes such as KRAS and EGFR, and tumor suppressor genes, such as TP53 [76]. Genome-wide CRISPR screens can identify new genetic markers associated with tumor aggressiveness, metastasis, and treatment resistance. These markers can be used to predict patient outcomes and personalize anti-cancer therapy. The biosensor can be designed with a sgRNA that targets a specific cancer biomarker sequence. The Cas9 enzyme, guided by the sgRNA, will bind to the target DNA sequence if present. The binding event can trigger a fluorescence change, an electrochemical signal, or a colorimetric change. These biosensors allow early rapid and sensitive detection of cancer by identifying the specific associated mutations or gene sequences [77]. Cas effectors in the Cas9, Cas12, Cas13 and Cas14 families have been used for biosensing purpose [78,79,80].
To provide more precise or conclusive information for molecular diagnostics, multiplex detection of several targets from a single tumor sample is currently in development [81, 82].
Applications of CRISPR/Cas9 to investigate the role of genes involved in carcinogenesis by functional genomics
CRISPR/Cas9 system can be used to understand gene function, at the single-cell level or in the context of an entire organism, observing the effects of its loss (gene knock-out), or the consequences of insertion or replacement of a specific gene or genetic sequence (gene knock-in) or the significance of modulating gene expression without altering the DNA sequence (gene activation, CRISPRa, and gene interference, CRISPRi) using dCas9 (which binds to, but does not cut DNA) fused with activation (VP64, p300) or repression (KRAB) domains to upregulate or downregulate target genes [83]. Selective activation or repression of genes can be used to investigate their impact on tumor growth and patient outcomes. Genome-wide screen by CRISPRa library in vivo for drivers of hepatocellular carcinoma (HCC) progression revealed that overexpression of XAGE1B, PLK4, LMO1 and MYADML2 genes promoted HCC cell proliferation and invasion, which were suppressed by their inhibition. Furthermore, high level of MYADML2 protein was associated with worse overall survival and reduced sensitivity to chemotherapeutic drugs [84].
CRISPR/Cas9 enables genome library screening approach, which can detect genes essential for cancer cell survival and drug resistance via Gain-Of-Function (GOF) or Loss-Of-Function (LOF). Genome-wide CRISPR/Cas9-mediated LOF screens in tumor and metastasis have discovered key genes involved in early, late and metastatic cancer [85, 86]. CRISPR/Cas9-based high-throughput LOF screening has identified farnesyltransferase among the top hits contributing to sunitinib resistance in clear cell renal cell carcinoma [87]. CRISPR/Cas9 screening platform have been used to identify genetic vulnerabilities in acute myeloid leukemia (AML) cells, including several established (such as DOT1L, BCL2, and MEN1) and novel (such as KAT2A) therapeutic targets for AML [88]. In vivo, genome-wide CRISPR LOF screen has identified TGFβ3 as an actionable biomarker of palbociclib resistance in triple negative breast cancer [89]. Genome-wide CRISPR screen in glioblastoma has identified loss of IFNγR signalling as a mechanism of resistance to CAR-T cell cytotoxicity [90]. Genome-scale CRISPR/Cas9 screening of 324 cancer cell lines from 30 cancer types, developed to provide an effective portfolio of cancer drug targets, has recently identified Werner syndrome ATP-dependent helicase (WRN) as a new candidate synthetic lethal target in microsatellite instability tumors [91].
In conclusion, CRISPR/Cas9 system can be used to identify cancer driving mutations, prognostic biomarkers [92,93,94] and therapeutic target genes, which are essential for precision medicine and personalized management of cancer patients.
Challenges to address
While the potential of CRISPR/Cas9 in cancer treatment and diagnosis is immense, several challenges remain. Issues to be addressed and strategies to overcome limitations of the CRISPR/Cas9 system in clinical applications involve: (a) Delivery methods. Efficient and targeted delivery of the CRISPR components (Cas9 protein and sgRNA) to specific cells and tissues is crucial. Current methods, such as viral vectors (e.g., AAV, lentivirus) and non-viral approaches (e.g., lipid nanoparticles), have limitations in terms of specificity, efficiency, and safety. Natural occurring AAV variants, which can be isolated from human and nonhuman primate tissues using high-cycle PCR and high-throughput sequencing [95] and directed evolution (which is an engineering approach to develop novel AAV variants with designated specificity, including random or defined peptide insertion, capsid shuffling, error-prone PCR, and saturation mutagenesis) are strategies currently employed for viral vector optimization which may reduce genotoxicity, and improve safety, tissue specificity, and packaging capacity [96]. Non-viral vectors, such as, lipid nanoparticles, which can encapsulate CRISPR/Cas9 components (and has proven particularly useful for delivering mRNA or protein forms of CRISPR/Cas9) and facilitate cellular uptake through endocytosis [97], and polymeric nanoparticles, which can be engineered to release their payload in response to specific stimuli (e.g., pH, enzymes) [98], can be functionalized with antibodies that specifically recognize and bind to tumor-associated antigens [99]. Gold nanoparticles offer a high degree of surface modification, allowing for the attachment of various targeting ligands [100]. Naturally occurring exosomes and extracellular vesicles, can carry CRISPR/Cas9 components to specific tissues, minimizing immune responses and reducing off-target effects [101,102,103]. Exosome-based CRISPR delivery systems are being studied for their ability to overcome blood-brain barrier and blood-brain tumor barrier to target glioblastoma cells [104, 105]; (b) Off-target effects. CRISPR can sometimes cut DNA at unintended sites, leading to off-target effects that cause unintended genetic modifications, which can be harmful and potentially increase cancer risks or create unwanted immune responses. Improving the specificity of the CRISPR system is essential to minimize these risks and can be achieved with the following methods: i) Enhancing HDR efficiency with small molecules, such as HDR enhancers (e.g., RS-1, a stimulator of RAD51, a DNA repair protein, ref. [106]), to increase the proportion of cells undergoing HDR [107]; ii) Using cell cycle regulators (cyclin-dependent kinase inhibitors, checkpoint kinase 1 inhibitors, aurora kinase inhibitors, such as VX-680 – Tozasertib, which block cells in the G2/M phase) to transiently push cells into HDR-active phases and make CRISPR/Cas9 editing less effective in non-dividing or slowly dividing cells [108]; iii) Improving sgRNA design by incorporating modified nucleotides or chemical modifications in sgRNAs [109] to enhance binding specificity and stability [110], as obtained in human primary T cells and CD34+ hematopoietic stem and progenitor cells [111], and by using artificial intelligence (AI)-powered bioinformatics tools, such as DeepCRISPR [112] and CRISPR-DO [113, 114]. These machine learning algorithms have been developed to predict the efficiency and specificity of guide RNAs and are instrumental in designing gRNAs that maximize on-target efficacy and minimize off-target risks, leading to safer CRISPR applications, especially for therapeutic uses; iv) Improving the enzyme’s specificity by using high-fidelity Cas9 variants, like eSpCas9 [115], HypaCas9 [116] and SpCas9-HF1 [117], which have been engineered (via mutations that reduce their binding to off-target sites) to reduce unintentional cuts in the genome and prevent unintended genetic changes [118, 119]; v) Using base editors, like CRISPR/Cas9 fused to deaminases, which enable direct chemical alteration of a single DNA base without creating double-stranded breaks, allowing for precise editing at the single-base level which is crucial for treating point mutations [120]; vi) Applying prime editing, which has been developed to generate targeted point mutations, as well as insertions or deletions in an HDR-independent manner [121] and consists of a prime editing guide RNA and a fusion protein construct composed of Cas9 nickase (a modified version of the CRISPR/Cas9 protein, engineered to create single-strand “nicks” in DNA rather than the typical double-strand break, DSB, that standard Cas9 produces) with an inactivated HNH domain and an engineered reverse transcriptase domain [122]. This approach reduces the likelihood of off-target effects and offers a broader range of genetic modifications [123]; vii) Applying advanced screening techniques for off-target detection, such as GUIDE-seq [124] and Digenome-seq [125], which are sequencing-based methods used to identify off-target effects by mapping unintended DNA cuts. GUIDE-seq and Digenome-seq help evaluate the precision of CRISPR edits and refine gRNA designs to reduce off-target activity. CHANGE-seq is a simplified, sensitive and automatable tagmentation-based method for measuring the genome-wide activity of Cas9 to understand the specificity of genome editors [126]. CIRCLE-seq is a newer, rapid and more sensitive technique that detects off-target effects by sequencing circular DNA fragments, providing an accurate measure of unintended DNA breaks [127, 128]; (c) Immune Response to CRISPR Components. Cas9 derived from bacterial species like Streptococcus pyogenes (SpCas9) and Staphylococcus aureus (SaCas9), which the human immune system may recognize as foreign (through pattern recognition receptors (PRRs), triggering inflammation and cytokine release) leads to unwanted innate and adaptive cellular immune responses [129]. The risk of such adverse reactions can be minimized by 1. Using less immunogenic Cas9 variants from less common bacterial strains [130], which can be selected with prediction models [131], or orthologs with low immunogenicity from non-pathogenic bacteria, such as Cas9 from Geobacillus stearothermophilus, which was found to be highly stable in human plasma [132]. 2. Delivering Cas9 transiently, e.g., as mRNA or protein, rather than DNA, limits its expression duration, reducing exposure to the immune system [133, 134]. 3. Humanizing Cas9 Protein, through the incorporation of sequences or motifs that mimic human proteins and can reduce immune recognition [135, 136]. 4. Using less immunogenic delivery systems, such as lipid nanoparticles or polymer-based carriers to shield Cas9 from immune recognition [97,98,99]; (d) Ethical and regulatory issues. Although developing anti-cancer treatments using CRISPR focus on somatic cells, ensuring that CRISPR is restricted to these cells can be challenging. Germline editing, which would be passed on to future generations, raises ethical concerns. Strong ethical guidelines and regulatory frameworks, possibly overseen by international bodies like the WHO, need to be established to ensure the safe and ethical use of CRISPR in humans [137, 138]. Transparent public engagement, that involves encouraging open dialogue with the public about the benefits, risks, and ethical issues of CRISPR technology, can improve understanding and trust of potential patients. Prioritizing research on CRISPR technologies and promoting health policies for equitable access to cutting-edge treatments and diagnostics could reduce social disparities in accessing up-to-date health care.
Current clinical trials testing CRISPR/Cas9-based antitumor therapeutic strategies are reported in Table 2 [139]. Meanwhile, research applying CRISPR systems based on different enzymatic proteins, such as Cas12 and Cas 13, is gaining ground.
Opportunities for cancer diagnosis and treatment using the novel Cas12- and Cas13-based CRISPR systems
Discovery of alternative CRISPR systems beyond the widely used Type II Streptococcus pyogenes Cas9 has expanded the toolkit for genetic manipulation.
CRISPR/Cas12 is a member of the CRISPR gene-editing family, which belongs to the Class 2, Type V system, with Cas12a being one of its most used subtypes [3]. Cas12 recognizes complementary ssDNA or dsDNA containing a PAM sequence under the guidance of its CRISPR RNA (crRNA), which directs DNA cleavage through a single RuvC structural domain [140]. Cas12 has been reported to have efficient trans-cleavage activity. It can induce robust and nonspecific ssDNA cleavage when it cleaves dsDNA in a sequence-specific manner, a property that has been widely used, especially in diagnostic applications, since its discovery in 2018 [141]. CRISPR/Cas12 can induce double-stranded breaks (DSBs) for permanent gene knock-out, insertion, or correction (Fig. 1b). Compared to Cas9, Cas12 has important advantages, such as: 1. generating staggered or “sticky” ends in DNA, which can enhance homology-directed repair and be advantageous in precision genome editing [142]; 2. targeting several distinct genomic loci, a process referred to as multiplexing, which enables strategies for targeting diseases involving multiple genes [143]; 3. the property of non-specific single-strand DNA cleavage activity, which makes Cas12 suitable for molecular diagnostics, such as detecting specific DNA sequences in infectious diseases and cancers [144].
CRISPR/Cas13 is another member of the CRISPR family of technologies, but it stands out because it targets RNA rather than DNA. Cas13, which belongs to the Class 2, Type VI system, contains the HEPN structural domain that binds to RNA for cleavage and is guided by a single RNA [145]. Cas13a (formerly C2c2) is one of its widely used subtypes [146]. It has been found that the Cas13a-crRNA complex, once activated by binding to its target RNA, cleaves it as well as other non-specific RNAs. This trans-cleavage capability expands the range of targets to be detected [19]. Since Cas13, unlike Cas9, binds to and cleaves single-stranded RNA molecules in a sequence-specific manner, it can be safely used in situations where temporary gene expression regulation is desired, without altering the host genome [103, 147] (Fig. 1c), which makes Cas13 a versatile tool for detecting viral- or cancer-related RNA sequences for molecular diagnostics [147]. Compared to Cas9, which typically affects only its target DNA site directly and does not have collateral activity, Cas13 has a unique collateral activity meaning that after it binds to its target RNA and being activated, it can nonspecifically cleave other RNAs nearby, a feature exploited in sensitive diagnostic techniques, but to be carefully managed in therapeutic applications [refs 4, 148].
Combined applications of Cas12 and Cas13, in tandem, are feasible and allow researchers to edit DNA and modulate RNA within the same system. CRISPR/Cas12 and CRISPR/Cas13 expand the toolkit available for genetic and molecular biology research, offering new possibilities for genome and transcriptome editing, as well as innovative diagnostic applications.

Illustration of DNA strand cleavage tools. (a) Cas9 cleaves DNA double strands to form blunt ends. (b) Cas12a cuts DNA double strands to form sticky ends. (c) Cas13a recognizes and cleaves RNA strands. PAM: protospacer adjacent motif. PFS: protospacer flanking sequence. sgRNA: single guide RNA
CRISPR/Cas12
CRISPR/Cas12 is an RNA-guided endonuclease similar to Cas9, with some key differences. CRISPR/Cas12a (Cpf1) is a CRISPR effector that controls target genes by recognizing thymine-rich PAM sequences. Cas12a has a higher sensitivity to mismatches in the guide RNA than does Cas9, therefore, off-target sequence recognition and cleavage are lower [148]. The main features of CRISPR/Cas12 system are the following: (a) Single-strand nicking. Cas12 can create a single-strand break or “nick” in the DNA, which can be useful for more precise genome editing and reduced off-target effects compared to double-stranded breaks; (b) PAM sequence. Cas12 recognizes a different PAM sequence than Cas9, expanding the range of targetable DNA sequences; (c) Collateral cleavage activity. Once activated by binding to the target DNA, Cas12 exhibits nonspecific cleavage activity on ssDNA. This property is harnessed in diagnostic applications [149].
Applications of CRISPR/Cas12 system include: (a) Genome editing. Similarly to Cas9, Cas12 can be used for gene knock-outs, insertions, or substitutions. Its ability to make single-stranded nicks allows for more precise edits; (b) Gene regulation. Cas12 can be modified to regulate gene expression without cutting DNA, by using dCas12, a catalytically inactive nuclease; (c) Diagnostics. The collateral cleavage activity of Cas12 is used in diagnostic assays like DETECTR (DNA Endonuclease Targeted CRISPR Trans Reporter), where it can detect specific DNA sequences, with high sensitivity, by cleaving reporter molecules upon target recognition [150].
Applications of CRISPR/Cas12 in cancer research and treatment
Unlike Cas9, Cas12 can cleave both ssDNA and dsDNA, and it has unique properties that can be advantageous for certain applications in oncology, such as those described below.
-
1.
Gene editing. CRISPR/Cas12 can be used to edit genes that are involved in cancer development and progression. The intra-tumoral delivery of an oncolytic Adenovirus (oAd) co-expressing Cas12a and a crRNA targeting the Epidermal Growth Factor Receptor (EGFR) gene (oAd/Cas12a/crEGFR) in lung cancer cells has proven to induce efficient and precise editing of the targeted EGFR gene in a cancer-specific manner, without detectable off-target nuclease activity and elicited a potent antitumor effect via induction of apoptosis and inhibition of proliferation in cancer cells, ultimately leading to tumor regression [151]. The multiplex gene targeting capability of Cas12a were exploited to delete three frequently mutated genes, such as TP53, Adenomatous polyposis coli (APC), and Phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha gene (PIK3CA) simultaneously, in colorectal cancer patients [152]. CRISPR/Cas multiplex biosensing is currently being developed by coupling different Cas12a-crRNA complexes, which detect several targets in parallel from a single tumor sample, with conversion of targeted information into colorimetric signals [153].These studies have highlighted the unique advantages of Cas12a in therapeutic editing for cancer cells.
-
2.
Targeted therapies. CRISPR/Cas12 can be used to develop targeted cancer therapies. For instance, it can be used to introduce the CAR gene into T cells at specific locations within the genome and generate CAR-T cells with enhanced specificity and efficacy against cancer cells [154]. Beyond introducing the CAR gene, CRISPR/Cas12 can be used to knock-out the PD-1 gene preventing T cells from becoming exhausted and allowing them to maintain their cancer-fighting activity for longer periods [155]. Traditional methods of producing CAR-T cells often involve viral vectors, which can integrate randomly into the genome, potentially leading to mutations and cancer. CRISPR/Cas12 provides a more controlled and safer alternative, with the ability to target specific genes with minimal off-target effects [156].
-
3.
Synthetic lethality (SL) approaches. Synthetic lethality occurs when the simultaneous impairment of two genes leads to cell death, whereas the dysfunction of either gene alone does not. In cancer therapy, this concept is used to selectively kill cancer cells by targeting a gene that becomes essential for survival due to the mutation or loss of another gene that is already compromised in the cancer cell. In tumor harboring a mutation in one of these genes, targeting the partner gene, which is functional, can induce death in cancer cells, but leave unaffected normal cells, in which neither gene is typically mutated. CRISPR/Cas12 can be used to identify synthetic lethality interactions (SLI) in cancer cells, by targeting specific genes that, when simultaneously inhibited along with existing mutations, can lead to cancer cell death while sparing normal cells [157]. By identifying synthetic lethal partners of mutations that are common in certain cancers CRISPR/Cas12 can help identify new drug targets. For instance, BRCA1 or BRCA2 mutations in breast and ovarian cancers. Since PARP enzymes are involved in repairing single-strand breaks in DNA, inhibiting PARP in cells with BRCA1 or BRCA2 mutations leads to the accumulation of DNA damage, ultimately causing cell death. Ataxia Telangiectasia and Rad3-related protein, ATR, and Checkpoint Kinase 1, CHK1, are involved in DNA damage response. In TP53-mutant ovarian cancer cells, targeting the ATR/CHK1 pathway can lead to an accumulation of DNA damage and cell death, making ATR and CHK1 inhibitors promising therapeutic targets [158]. Drugs that inhibit the synthetic lethal partner gene could selectively kill cancer cells while sparing normal cells. CRISPR/Cas12 can be used to identify effective combination therapies by revealing which gene knock-outs (and thus potential drug targets) are synthetic lethal with existing cancer therapies [159]. This can lead to the development of combination treatments that are more effective and have fewer side effects.
-
4.
Cancer diagnostics. Cas12 has been harnessed for diagnostic purposes, due to its collateral cleavage activity, where it non-specifically cleaves ssDNA upon activation. This property is exploited in diagnostic assays to detect cancer biomarkers with high sensitivity and specificity [160, 161]. Cas12 can be programmed to detect specific mutations in oncogenes or tumor suppressor genes associated with different types of cancer. For instance, Cas12-based assays can identify mutations in genes like KRAS [162], TP53 [160], and BRAF [163], which are commonly mutated in cancers such as lung, colon, and melanoma. Cas12 can detect even low concentrations of ctDNA in liquid biopsies with high specificity, enabling early detection of cancer and monitoring of minimal residual disease. Coupled with an electrochemical biosensor with a low detection limit of 2 cells/mL, CRISPR/Cas12a system has been used to develop highly sensitive nucleic acid-based analytical [164].
In summary, CRISPR/Cas12 represents a powerful tool in advancing knowledge on the molecular basis of cancer, with potential applications ranging from gene editing and diagnostics to the development of targeted therapies. However, its clinical implementation requires overcoming technical, ethical, and regulatory hurdles.
DETECTR for cancer detection
DNA Endonuclease-Targeted CRISPR Trans Reporter (DETECTR) is another CRISPR-based diagnostic platform, akin to Specific High Sensitivity Enzymatic Reporter UnLOCKing (SHERLOCK), developed for the rapid and accurate detection of specific nucleic acid sequences [150]. Leveraging the CRISPR/Cas12 system, DETECTR, which achieves attomolar sensitivity for DNA detection, has shown great potential in different applications, such as infectious disease diagnostics, genetic testing and cancer diagnostics [79].
The main features of DETECTR assay are the following: (a) Signal amplification. The collateral cleavage activity of Cas12 enzyme, that indiscriminately cuts nearby ssDNA reporters, results in amplified signal detection, enhancing sensitivity and enabling the detection of low-abundance targets, tumor DNA, or cancer-related viruses, in tissue samples and bodily fluids (e.g., blood, saliva, urine) from patients, facilitating early diagnosis and enabling precision medicine approaches. DETECTR can be adapted to detect various cancer-related mutations, such as those in oncogenes (e.g., KRAS, BRAF) or tumor suppressor genes (e.g., TP53), after detecting circulating tumor DNA (ctDNA) in blood samples. For viruses associated with cancer (e.g., Human Papillomavirus (HPV16 and HPV18) [165], Hepatitis B Virus (HBV), or Epstein-Barr Virus (EBV), the DETECTR assay targets specific viral sequences. Similarly to tumor DNA detection, the Cas12a protein is guided to the viral DNA or RNA sequence. Upon recognition, Cas12a is activated [166]. DETECTR can be tailored to detect multiple biomarkers simultaneously, providing a personalized profile of a patient’s cancer; (b) Specificity for target sequence and programmable specificity. The use of CRISPR/Cas12a ensures that the assay specifically detects the intended target without cross-reactivity with non-target sequences, reducing false positives [165]. The guide RNA (gRNA) used in the DETECTR is customizable and allows the assay to be programmed to recognize virtually any nucleic acid sequence and detect specific targets of interest across different applications; (c) Speed and simplicity. DETECTR provides accurate and rapid results, often within an hour or even minutes, which allows for faster decision-making in clinical settings. Furthermore, it can be performed with relatively simple equipment, low estimated cost and sustainable cost-benefit ratio. This makes it suitable for both clinical laboratories and point-of-care settings [165]; (d) Versatility. Like SHERLOCK, DETECTR can be adapted to detect a variety of nucleic acid targets, making it applicable for multiple types of cancer biomarkers. While DETECTR is primarily designed for DNA detection, it can also be adapted for RNA targets by incorporating a reverse transcription step, converting RNA to complementary DNA (cDNA) before detection [167]; (e) Monitoring disease progression and treatment response. By tracking the levels of specific cancer-related DNA mutations or methylation patterns during treatment, DETECTR can help assess the effectiveness of therapy and detect early signs of recurrence.
Despite the advantages it could provide, several challenges must be addressed to move the DETECTR platform into the clinical setting, such as: 1. carrying out clinical trials and validation studies to confirm the accuracy, the sensitivity, and the specificity of DETECTR for different types of cancer and patient populations; 2. integration of DETECTR within the existing diagnostic frameworks and compliance with regulatory standards; 3. ensuring the reliability of DETECTR addressing potential issues with false positives and negatives, which can impact clinical decisions.
In conclusion, DETECTR represents a significant advancement in cancer diagnostics, offering a rapid, sensitive, and cost-effective method for detecting cancer-related genetic mutations and biomarkers. Its application in non-invasive liquid biopsies and real-time monitoring of disease progression holds the promise of improving early cancer detection, treatment outcomes, and overall patient care.
CRISPR/Cas13
CRISPR/Cas13 is an RNA-guided RNA endonuclease that specifically targets RNA molecules instead of DNA. Upon binding to a target RNA sequence, Cas13 then cleaves the RNA, which can be used for various applications involving RNA manipulation [148].
The main features of CRISPR/Cas13 system are the following: (a) RNA targeting. Unlike Cas9 and Cas12, which target DNA, Cas13 specifically binds to and cleaves RNA molecules. This makes it an excellent tool for post-transcriptional regulation; (b) Collateral cleavage activity. Similarly to Cas12, Cas13 also exhibits collateral cleavage activity, but it targets RNA instead of DNA, which makes it useful for RNA detection assays [148]; (c) Programmability. Cas13 can be programmed with a specific guide RNA to target any RNA sequence, allowing the precise manipulation of RNA.
Applications of CRISPR/Cas13 system include: (a) RNA knock-down. Cas13 can be used to degrade specific RNA molecules, thereby reducing the expression of target genes at the RNA level. This property is useful for studying gene function and for therapeutic applications where reduction of harmful RNA is desired [168]; (b) RNA editing. By fusing Cas13 with RNA-editing enzymes, researchers can achieve precise RNA editing, which can be beneficial for correcting RNA transcripts without altering the genome [168]; (c) Diagnostics. The collateral cleavage activity of Cas13 can be exploited in diagnostic platforms like SHERLOCK, which can detect specific RNA sequences with high sensitivity and specificity. This feature allows the detection of viral RNA, as demonstrated for the detection of severe acute respiratory syndrome coronavirus 2 (SARS‑CoV‑2) [160].
Applications of CRISPR/Cas13 in cancer research and treatment
CRISPR/Cas13 has garnered significant attention for its potential applications in cancer research and treatment [169]. Unlike the more widely known CRISPR/Cas9, which targets DNA, CRISPR/Cas13 targets RNA, enabling the following approaches for cancer therapeutics and diagnostics.
-
1.
Knock-down of oncogenes and drug-resistant genes for therapeutic and discovery purposes.
-
a.
Therapeutic targeting of oncogenes and non-coding RNAs. By degrading the mRNA transcripts of oncogenes, CRISPR/Cas13 can reduce the expression of proteins that drive cancer cell proliferation and survival. Cas13a-based CRISPR system has proven effective in knocking down the expression of oncogenes, such as TERT, EZH2, and RelA, at both the mRNA and protein levels, in human hepatocarcinoma cells and tumor xenografts, leading to significant cancer cell apoptosis and tumor growth inhibition [170].
CRISPR/Cas13a-mediated knock-down of oncogenic KRASG12D mRNA expression in pancreatic cancer cells, revealed up to a 94% knock-down efficiency, with no detectable effects on wild-type KRAS mRNA, resulting in cancer cell apoptosis and marked tumor shrinkage [171]. These data support the use of CRISPR/Cas13a system as a flexible, targeted therapeutic tool.
Cas13 can also target non-coding RNAs, such as long non-coding RNAs (lncRNAs) and microRNAs (miRNAs), which play crucial roles in cancer progression [172, 173].
-
b.
Identifying cancer driver genes and therapeutic targets. CRISPR/Cas13 can be used in high-throughput screens to knock-down genes across the genome, helping identify genes that are essential for cancer cell survival [174]. CRISPR/Cas13-based knock-down screens in breast cancer cells has been used to identify breast cancer-risk associated lncRNAs, such as KILR, which, when knocked down, promotes DNA replication and cancer cell proliferation, when overexpressed, leads to cancer cell apoptosis [175].
-
c.
Identifying drug-resistant genes and mutations at the RNA level. Especially used to identify RNA transcripts from drug-resistant bacteria, viruses, or parasites by targeting specific resistance genes (e.g. those encoding beta-lactamases, efflux pumps, or viral polymerase mutations), Cas13 can also detect mRNA transcripts that relate to drug resistance in cancer cells and provides evidence supporting their biological significance. For instance, Cas13 could be used to detect deregulation of cAMP-regulatory element-binding protein (CREB) associated with resistance to carboplatin in metastatic breast cancer [176], multidrug resistance-associated protein 3 (MRP3) and multidrug resistance 1 (MDR1) genes associated to carboplatin resistance in NSCLC [176], and NRF2, TGFβ and TPp53 signaling associated with platinum-based chemotherapy resistance in ovarian cancer [176].
-
2.
Detection of specific RNA sequences associated with cancer for diagnostic applications. CRISPR/Cas13 system can be engineered to detect specific RNA sequences associated with cancer in the context of circulating (ct)RNA obtained from liquid biopsies (e.g. blood, urine) providing a minimally invasive method for early cancer detection and monitoring. The SHERLOCK platform, which utilizes CRISPR/Cas13, can detect cancer-related RNAs with high sensitivity and specificity [177].
CRISPR/Cas13’s ability to target RNA opens new avenues for gene downregulation, functional genomics, and diagnostics with potential benefit for public health [178, 179]. Overcoming the challenges related to delivery, specificity, and clinical translation is essential for realizing its full potential in oncology.
SHERLOCK for cancer detection
Originally developed for detecting viral and bacterial infections, SHERLOCK is an innovative diagnostic platform which uses CRISPR/Cas13 to detect cancer-related RNAs with high sensitivity and specificity [93, 177].
The main features of SHERLOCK assay are the following: (a) High sensitivity and specificity. SHERLOCK uses CRISPR/Cas systems, particularly Cas13 and Cas12, which can be programmed to target specific RNA or DNA sequences. It can detect and amplify very small quantities of nucleic acids (such as DNA or RNA) and identify genetic mutations associated with cancer enabling early diagnosis and accurate monitoring of treatment response. SHERLOCK’s sensitivity allows for the detection of cancer-related biomarkers in non-invasive liquid biopsies, such as blood, urine, or saliva [177]; (b) Versatility. SHERLOCK’s flexibility lies in its ability to detect a wide range of nucleic acids, including DNA, RNA, and microRNAs (miRNAs), which are key biomarkers in cancer. Different cancers are associated with specific genetic mutations, gene expression profiles, and epigenetic changes. SHERLOCK can be programmed to target and identify these diverse biomarkers, enabling the detection of multiple cancer types, even at early stages. One of SHERLOCK’s strengths is its ability to simultaneously detect multiple targets in a single assay, a process known as multiplexing. This feature is particularly useful in cancer diagnosis, where a single cancer type may be associated with several genetic mutations or alterations. By detecting multiple biomarkers in parallel, SHERLOCK can provide a more comprehensive profile of the cancer, aiding in more accurate diagnosis and personalized treatment planning; (c) Rapid results and cost-effectiveness. SHERLOCK can deliver results quickly, making it suitable for both clinical and point-of-care settings. Rapid detection is critical for early cancer diagnosis and timely treatment. Compared to traditional diagnostic methods like sequencing or imaging, SHERLOCK does not require extensive infrastructure or expensive equipment, and offers a more affordable option, improving accessibility to cancer screening and diagnostics.
Perspectives and challenges to overcome to move the SHERLOCK platform into the clinical setting
As required for the routine use of DETECTR, clinical trials and validation studies are needed to standardize SHERLOCK for cancer diagnostics and to ensure its reliability across diverse patient populations. As for DETECTR, integration within existing diagnostic frameworks along with scalability and accessibility are issues that need to be addressed in the near future. A summary of common features and differences between the two platforms are provided in Table 3.
Overall, SHERLOCK may advance cancer diagnostics, offering a rapid, sensitive, and cost-effective method for detecting genetic mutations and biomarkers associated with cancer. SHERLOCK could become an integral part of personalized medicine, improving early cancer detection, monitoring, and overall patient outcomes.
Active clinical trials testing therapeutic applications of the CRISPR/Cas12 or CRISPR/Cas13 systems
While several clinical trials testing the efficacy of CRISPR/Cas9 system, in particular immunotherapeutic approaches to different types of advanced tumors, are ongoing (https://clinicaltrials.gov) and recently reported [180], no trials are currently active to determine the potential therapeutic application of Cas12- or Cas13-based CRISPR systems in oncology. Two clinical studies are ongoing testing the use of CRISPR/Cas12. One concerns the treatment of Severe Sickle Cell Disease (SCD) (ID NCT04853576) (Table 4) [139], an inherited blood disorder involving a defective hemoglobin synthesis, due to a single base-pair point mutation in the β-globin gene, which may lead to multi-organ failure and affects millions of people throughout the world [181]; the other is aimed at exploiting CRISPR/Cas12 for treatment Transfusion-Dependent Beta Thalassemia (TDT) (ID NCT05444894), the most serious form of beta-thalassemia caused by mutations in the β-globin gene leading to ineffective erythropoiesis and chronic severe anemia [182]. Only one study is currently active that use CRISPR/Cas13-mediated RNA targeting, and it is focused on the treatment of neovascular Age-Related Macular Degeneration (AMD) (ID NCT06031727) (Table 4) [139], an acquired degeneration of the retina, which affects one in eight people 60 years of age or older and is the most common cause of irreversible blindness in older persons in developed countries [183].
Outstanding questions
What challenges must be overcome to move Cas12- and Cas13-based CRISPR systems into clinical oncology?
Moving Cas12- and Cas13-based CRISPR systems into clinical oncology presents challenges related to technical, safety, distribution, ethical, regulatory and translational research aspects, that must be overcome to harness their potential for cancer treatment [184]. Some of the key issues to be addressed are as follows.
-
Delivery mechanisms. Efficient and targeted delivery of Cas proteins and guide RNA to specific cells and tissues is crucial. Delivery methods need to ensure that Cas proteins and guide RNA reach the desired cells and tissues without causing off-target effects. Current delivery vectors, such as viral vectors (e.g. Adeno-Associated Virus, lentivirus) and non-viral methods (e.g. lipid nanoparticles) [185], have limitations, regarding specificity, efficiency, and safety, in ensuring effective systemic delivery of CRISPR components for metastatic cancers that have spread to multiple sites.
-
Off-target effects. Although Cas13 targets RNA rather than DNA, off-target effects are still a concern. Unintended RNA cleavage can disrupt normal cellular functions and lead to adverse effects. Improving the specificity of Cas13 to minimize off-target activity is essential.
-
Long-term effects and stability. Understanding the stability and long-term effects on patient health of DNA editing by Cas12, or RNA edits made by Cas13 is crucial for effective clinical applications. Efficacy and long-term safety represent major concerns that remain to be adequately addressed in preclinical studies [186].
-
Immunogenicity. All the components of CRISPR-based therapy, Cas9, Cas12 and Cas13 proteins, gRNA, viral or non-viral vectors, can elicit adverse immune reactions. Reducing their immunogenicity is essential to ensure the clinical availability and utility of CRISPR therapeutics [187].
-
Patient selection and genetic diversity. Patients’ genetic diversity can affect the success of both Cas12- and Cas13-based therapies [188, 189]. Personalized approaches may be required to account for variations in genetic backgrounds, which can influence the efficiency and safety of the treatment.
Overcoming these challenges through robust preclinical studies, rigorous clinical trials, multidisciplinary collaboration, and developing specific guidelines and standards for the use of CRISPR, will be crucial to provide opportunities for the successful clinical application of the next-generation CRISPR-based systems in modern precision oncology.
Data availability
No datasets were generated or analysed during the current study.
Abbreviations
- AAV:
-
adeno-associated virus
- AMD:
-
age-related macular degeneration
- CAR-T:
-
chimeric antigen receptor T cell
- Cas:
-
CRISPR-associated protein
- CRISPR:
-
clustered regularly interspaced short palindromic repeats
- crRNA:
-
CRISPR RNA
- CHANGE-seq:
-
circularization for high-throughput analysis of nuclease genome-wide effects by sequencing
- ctDNA:
-
circulating tumor DNA
- dCas:
-
nuclease-deficent Cas
- DETECTR:
-
DNA endonuclease targeted CRISPR trans reporter
- Digenome-seq:
-
Cas9 nuclease-digested whole genome sequencing
- DSB:
-
double-stranded break
- dsDNA/RNA:
-
double-stranded DNA/RNA
- GOF:
-
gain-of-function
- GUIDE-seq:
-
genome-wide unbiased identification of DSBs enabled by sequencing
- gRNA:
-
guide RNA
- HDR:
-
homology-directed repair
- lncRNA:
-
long non-coding RNAs
- Indels:
-
insertions-deletions
- LOF:
-
loss-of-function
- miRNA:
-
microRNA
- MDSCs:
-
myeloid-derived suppressor cells
- PAM:
-
protospacer adjacent motif
- PARPi:
-
poly(ADP-ribose) polymerase inhibitor
- PRRs:
-
pattern recognition receptors
- RS-1:
-
RAD51-stimulatory compound 1
- RuvC:
-
an endonuclease domain named for an E. coli protein involved in DNA repair
- SaCas9:
-
Staphylococcus aureus Cas9
- SCD:
-
severe sickle cell disease
- sgRNA:
-
single guide RNA
- SHERLOCK:
-
specific high sensitivity enzymatic reporter unLOCKing
- SpCas9:
-
Streptococcus pyogenes Cas9
- ssDNA/RNA:
-
single-stranded DNA/RNA
- TCR:
-
T cell receptor
- tracrRNA:
-
trans-activating crRNA
References
Faure G, Makarova KS, Koonin EV. CRISPR–Cas: Complex Functional Networks and multiple roles beyond adaptive immunity. J Mol Biol. 2019;431:3–20.
Jiang F, Doudna JA. CRISPR-Cas9 structures and mechanisms. Annu Rev Biophys. 2017;46:505–29.
Paul B, Montoya G. CRISPR-Cas12a: functional overview and applications. Biomed J. 2020;43:8–17.
Bot JF, van der Oost J, Geijsen N. The double life of CRISPR-Cas13. Curr Opin Biotechnol. 2022;78:102789.
Sternberg SH, Richter H, Charpentier E, Qimron U. Adaptation in CRISPR-Cas systems. Mol Cell. 2016;61:797–808.
Liu TY, Doudna JA. Chemistry of Class 1 CRISPR-Cas effectors: binding, editing, and regulation. J Biol Chem. 2020;295:14473–87.
Koonin EV, Makarova KS, Zhang F. Diversity, classification and evolution of CRISPR-Cas systems. Curr Opin Microbiol. 2017;37:67–78.
Makarova KS, Wolf YII, Iranzo J, Shmakov SA, Alkhnbashi OS, Brouns SJJ, et al. Evolutionary classification of CRISPR–Cas systems: a burst of class 2 and derived variants. Nat Rev Microbiol. 2020;18:67–83.
Gostimskaya I. CRISPR-Cas9: a history of its Discovery and ethical considerations of its Use in Genome Editing. Biochem (Mosc). 2022;87:777–88.
Ishino Y, Shinagawa H, Makino K, Amemura M, Nakata A. Nucleotide sequence of the iap gene, responsible for alkaline phosphatase isozyme conversion in Escherichia coli, and identification of the gene product. J Bacteriol. 1987;169:5429–33.
Mojica FJ, Juez G, Rodríguez-Valera F. Transcription at different salinities of Haloferax mediterranei sequences adjacent to partially modified PstI sites. Mol Microbiol. 1993;9:613–21.
Jansen R, Embden JD, Gaastra W, Schouls LM. Identification of genes that are associated with DNA repeats in prokaryotes. Mol Microbiol. 2002;43:1565–75.
Mojica FJ, Díez-Villaseñor C, García-Martínez J, Soria E. Intervening sequences of regularly spaced prokaryotic repeats derive from foreign genetic elements. J Mol Evol. 2005;60:174–82.
Jinek M, Chylinski K, Fonfara I, Hauer M, Doudna JA, Charpentier E. A programmable dual-RNA-guided DNA endonuclease in adaptive bacterial immunity. Science. 2012;337:816–21.
Cong L, Ran FA, Cox D, Lin S, Barretto R, Habib N, et al. Multiplex genome engineering using CRISPR/Cas systems. Science. 2013;339:819–23.
Mali P, Yang L, Esvelt KM, Aach J, Guell M, DiCarlo JE, et al. RNA-guided Hum Genome Eng via Cas9 Sci. 2013;339:823–6.
Makarova KS, Wolf YI, Alkhnbashi OS, Costa F, Shah SA, Saunders SJ, et al. An updated evolutionary classification of CRISPR-Cas systems. Nat Rev Microbiol. 2015;13:722–36.
Zetsche B, Gootenberg JS, Abudayyeh OO, Slaymaker IM, Makarova KS, Essletzbichler P, et al. Cpf1 is a single RNA-guided endonuclease of a class 2 CRISPR-Cas system. Cell. 2015;163:759–71.
Abudayyeh OO, Gootenberg JS, Konermann S, Joung J, Slaymaker IM, Cox DB, et al. C2c2 is a single-component programmable RNA-guided RNA-targeting CRISPR effector. Science. 2016;353:aaf5573.
Roth TL, Puig-Saus C, Yu R, Shifrut E, Carnevale J, Li PJ, et al. Reprogramming human T cell function and specificity with non-viral genome targeting. Nature. 2018;559:405–9.
Patel SJ, Sanjana NE, Kishton RJ, Eidizadeh A, Vodnala SK, Cam M, et al. Identification of essential genes for cancer immunotherapy. Nature. 2017;548:537–42.
Stadtmauer EA, Fraietta JA, Davis MM, Cohen AD, Weber KL, Lancaster E, et al. CRISPR-engineered T cells in patients with refractory cancer. Science. 2020;367:eaba7365.
Chen JS, Doudna JA. The chemistry of Cas9 and its CRISPR colleagues. Nat Rev Chem. 2017;1:0078.
O’Connell MR, Oakes BL, Sternberg SH, East-Seletsky A, Kaplan M, Doudna JA. Programmable RNA recognition and cleavage by CRISPR/Cas9. Nature. 2014;516:263–6.
Zhou W, Hu L, Ying L, Zhao Z, Chu PK, Yu X-F. A CRISPR–Cas9-triggered strand displacement amplification method for ultrasensitive DNA detection. Nat Commun. 2018;9:5012.
Jachowski A, Marcinkowski M, Szydłowski J, Grabarczyk O, Nogaj Z, Marcin Ł, et al. Modern therapies of nonsmall cell lung cancer. J Appl Genet. 2023;64(4):695–711.
Kim W, Lee S, Kim HS, Song M, Cha YH, Kim YH, et al. Targeting mutant KRAS with CRISPR-Cas9 controls tumor growth. Genome Res. 2018;28:374–82.
Liu B, Diaz Arguello OA, Chen D, Chen S, Saber A, Haisma HJ. CRISPR-mediated ablation of overexpressed EGFR in combination with sunitinib significantly suppresses renal cell carcinoma proliferation. PLoS ONE. 2020;15:e0232985.
Vuelta E, Ordoñez JL, Alonso-Pérez V, Méndez L, Hernández-Carabias P, Saldaña R, et al. CRISPR-Cas9 Technology as a Tool to target Gene drivers in Cancer: Proof of Concept and New opportunities to treat chronic myeloid leukemia. CRISPR J. 2021;4:519–35.
Martinez-Lage M, Torres-Ruiz R, Puig-Serra P, Moreno-Gaona P, Martin MC, Moya FJ, et al. In vivo CRISPR/Cas9 targeting of fusion oncogenes for selective elimination of cancer cells. Nat Commun. 2020;11:5060.
Pflanz S, Timans JC, Cheung J, Rosales R, Kanzler H, Gilbert J, et al. IL-27, a heterodimeric cytokine composed of EBI3 and p28 protein, induces proliferation of naive CD4 + T cells. Immunity. 2002;16:779–90.
D’Antonio L, Fieni C, Ciummo SL, Vespa S, Lotti L, Sorrentino C, et al. Inactivation of interleukin-30 in colon cancer stem cells via CRISPR/Cas9 genome editing inhibits their oncogenicity and improves host survival. J Immunother Cancer. 2023;11:e006056.
Sorrentino C, D’Antonio L, Ciummo SL, Fieni C, Landuzzi L, Ruzzi F, et al. CRISPR/Cas9-mediated deletion of Interleukin-30 suppresses IGF1 and CXCL5 and boosts SOCS3 reducing prostate cancer growth and mortality. J Hematol Oncol. 2022;15:145.
Sorrentino C, Ciummo SL, D’Antonio L, Fieni C, Lanuti P, Turdo A, et al. Interleukin-30 feeds breast cancer stem cells via CXCL10 and IL23 autocrine loops and shapes immune contexture and host outcome. J Immunother Cancer. 2021;9:e002966.
Di Meo S, Airoldi I, Sorrentino C, Zorzoli A, Esposito S, Di Carlo E. Interleukin-30 expression in prostate cancer and its draining lymph nodes correlates with advanced grade and stage. Clin Cancer Res. 2014;20:585–94.
Sorrentino C, Ciummo SL, Cipollone G, Caputo S, Bellone M, Di Carlo E. Interleukin-30/IL27p28 shapes prostate Cancer stem-like cell behavior and is critical for Tumor Onset and Metastasization. Cancer Res. 2018;78:2654–68.
Sorrentino C, Yin Z, Ciummo S, Lanuti P, Lu LF, Marchisio M, et al. Targeting interleukin(IL)-30/IL-27p28 signaling in cancer stem-like cells and host environment synergistically inhibits prostate cancer growth and improves survival. J Immunother Cancer. 2019;7:201.
Fieni C, Sorrentino C, Ciummo SL, Fontana A, Lotti LV, Scialis S, et al. Immunoliposome-based targeted delivery of the CRISPR/Cas9gRNA-IL30 complex inhibits prostate cancer and prolongs survival. Exp Mol Med. 2024 Sep;4. https://doi.org/10.1038/s12276-024-01310-2.
Fieni C, Ciummo SL, Sorrentino C, Marchetti S, Vespa S, Lanuti P, et al. Prevention of prostate Cancer metastasis by a CRISPR-delivering nanoplatform for Interleukin-30 genome editing. Mol Ther. 2024 Sep;6:S1525. 0016(24)00596-3.
Rafii S, Tashkandi E, Bukhari N, Al-Shamsi HO. Current status of CRISPR/Cas9 application in Clinical Cancer Research: opportunities and challenges. Cancers (Basel). 2022;14:947.
Fang N, Gu T, Wang Y, Wang S, Wang F, An Y, et al. Expression of PTEN-long mediated by CRISPR/Cas9 can repress U87 cell proliferation. J Cell Mol Med. 2017;21:3337–46.
Baylin SB, Jones PA. Epigenetic determinants of Cancer. Cold Spring Harb Perspect Biol. 2016;8:a019505.
Jones PA, Issa JP, Baylin S. Targeting the cancer epigenome for therapy. Nat Rev Genet. 2016;17:630–41.
Nakamura M, Gao Y, Dominguez AA, Qi LS. CRISPR technologies for precise epigenome editing. Nat Cell Biol. 2021;23:11–22.
Ansari I, Chaturvedi A, Chitkara D, Singh S. CRISPR/Cas mediated epigenome editing for cancer therapy. Semin Cancer Biol. 2022;83:570–83.
Kuang C, Park Y, Augustin RC, Lin Y, Hartman DJ, Seigh L, et al. Pembrolizumab plus azacitidine in patients with chemotherapy refractory metastatic colorectal cancer: a single-arm phase 2 trial and correlative biomarker analysis. Clin Epigenetics. 2022;14:3.
Contreras-Sanzón E, Prado-Garcia H, Romero-Garcia S, Nuñez-Corona D, Ortiz-Quintero B, Luna-Rivero C, et al. Histone deacetylases modulate resistance to the therapy in lung cancer. Front Genet. 2022;13:960263.
Tao L, Zhou Y, Luo Y, Qiu J, Xiao Y, Zou J, et al. Epigenetic regulation in cancer therapy: from mechanisms to clinical advances. MedComm – Oncol. 2024;3:e59.
Hamieh M, Mansilla-Soto J, Rivière I, Sadelain M. Programming CAR T cell tumor recognition: tuned Antigen Sensing and Logic Gating. Cancer Discov. 2023;13:829–43.
Liu Z, Shi M, Ren Y, Xu H, Weng S, Ning W, et al. Recent advances and applications of CRISPR-Cas9 in cancer immunotherapy. Mol Cancer. 2023;22:35.
Bexte T, Alzubi J, Reindl LM, Wendel P, Schubert R, Salzmann-Manrique E, et al. CRISPR-Cas9 based gene editing of the immune checkpoint NKG2A enhances NK cell mediated cytotoxicity against multiple myeloma. Oncoimmunology. 2022;11:2081415.
Tiash S, Chowdhury EH. siRNAs targeting multidrug transporter genes sensitise breast tumour to doxorubicin in a syngeneic mouse model. J Drug Target. 2019;27:325–37.
Lei ZN, Tian Q, Teng QX, Wurpel JND, Zeng L, Pan Y et al. Understanding and targeting resistance mechanisms in cancer. MedComm (2020). 2023;4:e265.
McLean B, Istadi A, Clack T, Vankan M, Schramek D, Neely GG, et al. A CRISPR path to finding vulnerabilities and solving Drug Resistance: targeting the Diverse Cancer Landscape and its ecosystem. Adv Genet (Hoboken). 2022;3:2200014.
Rupp LJ, Schumann K, Roybal KT, Gate RE, Ye CJ, Lim WA, et al. CRISPR/Cas9-mediated PD-1 disruption enhances anti-tumor efficacy of human chimeric antigen receptor T cells. Sci Rep. 2017;7:737.
Benjamin R, Graham C, Yallop D, Jozwik A, Mirci-Danicar OC, Lucchini G, et al. Genome-edited, donor-derived allogeneic anti-CD19 chimeric antigen receptor T cells in paediatric and adult B-cell acute lymphoblastic leukaemia: results of two phase 1 studies. Lancet. 2020;396:1885–94.
Lu S, Yang N, He J, Gong W, Lai Z, Xie L, et al. Generation of CancerSpecific cytotoxic PD-1(-) T cells using Liposome-Encapsulated CRISPR/ Cas System with Dendritic/Tumor Fusion cells. J BioMed Nanotechnol. 2019;15:593–601.
Pomeroy EJ, Hunzeker JT, Kluesner MG, Lahr WS, Smeester BA, Crosby MR, et al. A genetically Engineered Primary Human Natural Killer Cell platform for Cancer Immunotherapy. Mol Ther. 2020;28:52–63.
Vaghari-Tabari M, Hassanpour P, Sadeghsoltani F, Malakoti F, Alemi F, Qujeq D, et al. CRISPR/Cas9 gene editing: a new approach for overcoming drug resistance in cancer. Cell Mol Biol Lett. 2022;27:49.
Dhanyamraju PK. Drug resistance mechanisms in cancers: execution of pro-survival strategies. J Biomed Res. 2024;38:95–121.
Liao S, Davoli T, Leng Y, Li MZ, Xu Q, Elledge SJ. A genetic interaction analysis identifies cancer drivers that modify EGFR dependency. Genes Dev. 2017;31:184–96.
Sun W, He B, Yang B, Hu W, Cheng S, Xiao H, et al. Genome-wide CRISPR screen reveals SGOL1 as a druggable target of sorafenib-treated hepatocellular carcinoma. Lab Invest. 2018;98:734–44.
Goodspeed A, Jean A, Costello JC. A whole-genome CRISPR screen identifies a role of MSH2 in cisplatin-mediated cell death in muscle-invasive bladder Cancer. Eur Urol. 2019;75:242–50.
Ha JS, Byun J, Ahn DR. Overcoming doxorubicin resistance of cancer cells by Cas9-mediated gene disruption. Sci Rep. 2016;6:22847.
Yang Y, Qiu JG, Li Y, Di JM, Zhang WJ, Jiang QW, et al. Targeting ABCB1-mediated tumor multidrug resistance by CRISPR/Cas9-based genome editing. Am J Transl Res. 2016;8:3986–94.
Rocha CRR, Reily Rocha A, Molina Silva M, Rodrigues Gomes L, Teatin Latancia M, Andrade Tomaz M, et al. Revealing Temozolomide Resistance mechanisms via genome-wide CRISPR libraries. Cells. 2020;9:2573.
Farmer H, McCabe N, Lord CJ, Tutt AN, Johnson DA, Richardson TB, et al. Targeting the DNA repair defect in BRCA mutant cells as a therapeutic strategy. Nature. 2005;434:917–21.
Tsujino T, Takai T, Hinohara K, Gui F, Tsutsumi T, Bai X, et al. CRISPR screens reveal genetic determinants of PARP inhibitor sensitivity and resistance in prostate cancer. Nat Commun. 2023;14:252.
Miao C, Tsujino T, Takai T, Gui F, Tsutsumi T, Sztupinszki Z, et al. RB1 loss overrides PARP inhibitor sensitivity driven by RNASEH2B loss in prostate cancer. Sci Adv. 2022;8:eabl9794.
Tian Y, Lei Y, Wang Y, Lai J, Wang J, Xia F. Mechanism of multidrug resistance to chemotherapy mediated by P–glycoprotein (review). Int J Oncol. 2023;63:119.
Xu Y, Zhu M. Novel exosomal miR-46146 transfer oxaliplatin chemoresistance in colorectal cancer. Clin Transl Oncol. 2020;22:1105–16.
Mohammadzadeh I, Qujeq D, Yousefi T, Ferns GA, Maniati M, Vaghari-Tabari M. CRISPR/Cas9 gene editing: a new therapeutic approach in the treatment of infection and autoimmunity. IUBMB Life. 2020;72:1603–21.
Liu S, Chen S, Yuan W, Wang H, Chen K, Li D, et al. PD-1/PD-L1 interaction up-regulates MDR1/P-gp expression in breast cancer cells via PI3K/AKT and MAPK/ERK pathways. Oncotarget. 2017;8:99901–12.
Wu X, Li Y, Liu X, Chen C, Harrington SM, Cao S, et al. Targeting B7—H1 (PD—L1) sensitizes Cancer cells to Chemotherapy. Heliyon. 2018;4:e01039.
Chen M, Wu D, Tu S, Yang C, Chen D, Xu Y. CRISPR/Cas9 cleavage triggered ESDR for circulating tumor DNA detection based on a 3D graphene/AuPtPd nanoflower biosensor. Biosens Bioelectron. 2021;173:112821.
Liu CC, Dai Y. Application of CRISPR Cas systems for Biosensing. Biosens (Basel). 2023;13:672.
Chen K, Shen Z, Wang G, Gu W, Zhao S, Lin Z, et al. Research progress of CRISPR-based biosensors and bioassays for molecular diagnosis. Front Bioeng Biotechnol. 2022;10:986233.
Gootenberg JS, Abudayyeh OO, Kellner MJ, Joung J, Collins JJ, Zhang F. Multiplexed and portable nucleic acid detection platform with Cas13, Cas12a, and Csm6. Science. 2018;360:439–44.
Chen JS, Ma E, Harrington LB, Da Costa M, Tian X, Palefsky JM, et al. CRISPR-Cas12a target binding unleashes indiscriminate single-stranded DNase activity. Science. 2018;360:436–9.
Bruch R, Urban GA, Dincer C. CRISPR/Cas Powered Multiplexed Biosensing. Trends Biotechnol. 2019;37:791–2.
Kumaran A, Jude Serpes N, Gupta T, James A, Sharma A, Kumar D, et al. Advancements in CRISPR-Based Biosensing for Next-Gen Point of Care Diagnostic Application. Biosens (Basel). 2023;13:202.
Karlikow M, Amalfitano E, Yang X, Doucet J, Chapman A, Mousavi PS, et al. CRISPR-induced DNA reorganization for multiplexed nucleic acid detection. Nat Commun. 2023;14:1505.
Wang LW, Trudeau SJ, Wang C, Gerdt C, Jiang S, Zhao B et al. Modulating Gene Expression in Epstein-Barr Virus (EBV)-Positive B Cell Lines with CRISPRa and CRISPRi. Curr Protoc Mol Biol. 2018;121:31.13.1-31.13.18.
Zhang B, Ren Z, Zheng H, Lin M, Chen G, Luo OJ, et al. CRISPR activation screening in a mouse model for drivers of hepatocellular carcinoma growth and metastasis. iScience. 2023;26:106099.
Chen S, Sanjana NE, Zheng K, Shalem O, Lee K, Shi X, et al. Genome-wide CRISPR screen in a mouse model of tumor growth and metastasis. Cell. 2015;160:1246–60.
Kiessling MK, Schuierer S, Stertz S, Beibel M, Bergling S, Knehr J, et al. Identification of oncogenic driver mutations by genome-wide CRISPR-Cas9 dropout screening. BMC Genomics. 2016;17:723.
Makhov P, Sohn JA, Serebriiskii IG, Fazliyeva R, Khazak V, Boumber Y, et al. CRISPR/Cas9 genome-wide loss-of-function screening identifies druggable cellular factors involved in sunitinib resistance in renal cell carcinoma. Br J Cancer. 2020;123:1749–56.
Tzelepis K, Koike-Yusa H, De Braekeleer E, Li Y, Metzakopian E, Dovey OM, et al. A CRISPR dropout screen identifies genetic vulnerabilities and therapeutic targets in Acute myeloid leukemia. Cell Rep. 2016;17:1193–205.
Poulet S, Dai M, Wang N, Yan G, Boudreault J, Daliah G, et al. Genome-wide in vivo CRISPR screen identifies TGFβ3 as actionable biomarker of palbociclib resistance in triple negative breast cancer. Mol Cancer. 2024;23:118.
Larson RC, Kann MC, Bailey SR, Haradhvala NJ, Llopis PM, Bouffard AA, et al. CAR T cell killing requires the IFNγR pathway in solid but not liquid tumours. Nature. 2022;604:563–70.
Behan FM, Iorio F, Picco G, Gonçalves E, Beaver CM, Migliardi G, et al. Prioritization of cancer therapeutic targets using CRISPR-Cas9 screens. Nature. 2019;568:511–6.
Ng SR, Rideout WM 3rd, Akama-Garren EH, Bhutkar A, Mercer KL, Schenkel JM, et al. CRISPR-mediated modeling and functional validation of candidate tumor suppressor genes in small cell lung cancer. Proc Natl Acad Sci U S A. 2020;117:513–21.
Shi X, Kitano A, Jiang Y, Luu V, Hoegenauer KA, Nakada D. Clonal expansion and myeloid leukemia progression modeled by multiplex gene editing of murine hematopoietic progenitor cells. Exp Hematol. 2018;64:33–e445.
Takeda H. A platform for validating Colorectal Cancer driver genes using mouse organoids. Front Genet. 2021;12:698771.
Srivastava A. Rationale and strategies for the development of safe and effective optimized AAV vectors for human gene therapy. Mol Ther Nucleic Acids. 2023;32:949–59.
Wang JH, Gessler DJ, Zhan W, Gallagher TL, Gao G. Adeno-associated virus as a delivery vector for gene therapy of human diseases. Signal Transduct Target Ther. 2024;9:78.
Mohammadian Farsani A, Mokhtari N, Nooraei S, Bahrulolum H, Akbari A, Farsani ZM, et al. Lipid nanoparticles: the game-changer in CRISPR-Cas9 genome editing. Heliyon. 2024;10:e24606.
Ashok B, Peppas NA, Wechsler ME. Lipid- and polymer-based Nanoparticle systems for the delivery of CRISPR/Cas9. J Drug Deliv Sci Technol. 2021;65:102728.
Marques AC, Costa PC, Velho S, Amaral MH. Lipid nanoparticles functionalized with antibodies for Anticancer Drug Therapy. Pharmaceutics. 2023;15:216.
Kanu GA, Parambath JBM, Abu Odeh RO, Mohamed AA. Gold nanoparticle-mediated gene therapy. Cancers (Basel). 2022;14:5366.
Liang Y, Iqbal Z, Wang J, Xu L, Xu X, Ouyang K, et al. Cell-derived extracellular vesicles for CRISPR/Cas9 delivery: engineering strategies for cargo packaging and loading. Biomater Sci. 2022;10:4095–106.
Ilahibaks NF, Kluiver TA, de Jong OG, de Jager SCA, Schiffelers RM, Vader P, et al. Extracellular vesicle-mediated delivery of CRISPR/Cas9 ribonucleoprotein complex targeting proprotein convertase subtilisin-kexin type 9 (Pcsk9) in primary mouse hepatocytes. J Extracell Vesicles. 2024;13:e12389.
Dubey S, Chen Z, Jiang YJ, Talis A, Molotkov A, Ali A, et al. Small extracellular vesicles (sEVs)-based gene delivery platform for cell-specific CRISPR/Cas9 genome editing. Theranostics. 2024;14:2777–93.
Khatami SH, Karami N, Taheri-Anganeh M, Taghvimi S, Tondro G, Khorsand M, et al. Exosomes: Promising Delivery Tools for overcoming blood-brain barrier and Glioblastoma therapy. Mol Neurobiol. 2023;60:4659–78.
Zhu Q, Ling X, Yang Y, Zhang J, Li Q, Niu X, et al. Embryonic stem cells-derived exosomes endowed with Targeting properties as Chemotherapeutics Delivery vehicles for Glioblastoma Therapy. Adv Sci (Weinh). 2019;6:1801899.
Song J, Yang D, Xu J, Zhu T, Chen YE, Zhang J. RS-1 enhances CRISPR/Cas9- and TALEN-mediated knock-in efficiency. Nat Commun. 2016;7:10548.
Lee ABC, Tan MH, Chai CLL. Small-molecule enhancers of CRISPR-induced homology-directed repair in gene therapy: a medicinal chemist’s perspective. Drug Discov Today. 2022;27:2510–25.
Li G, Yang X, Luo X, Wu Z, Yang H. Modulation of cell cycle increases CRISPR-mediated homology-directed DNA repair. Cell Biosci. 2023;13:215.
Ryan DE, Taussig D, Steinfeld I, Phadnis SM, Lunstad BD, Singh M, et al. Improving CRISPR-Cas specificity with chemical modifications in single-guide RNAs. Nucleic Acids Res. 2018;46:792–803.
Guo C, Ma X, Gao F, Guo Y. Off-target effects in CRISPR/Cas9 gene editing. Front Bioeng Biotechnol. 2023;11:1143157.
Hendel A, Bak RO, Clark JT, Kennedy AB, Ryan DE, Roy S, et al. Chemically modified guide RNAs enhance CRISPR-Cas genome editing in human primary cells. Nat Biotechnol. 2015;33:985–9.
Chuai G, Ma H, Yan J, Chen M, Hong N, Xue D, et al. DeepCRISPR: optimized CRISPR guide RNA design by deep learning. Genome Biol. 2018;19:80.
Ma J, Köster J, Qin Q, Hu S, Li W, Chen C, et al. CRISPR-DO for genome-wide CRISPR design and optimization. Bioinformatics. 2016;32:3336–8.
Barozzi I, Slaven N, Canale E, Lopes R, Amorim Monteiro Barbosa I, Bleu M, et al. A functional survey of the Regulatory Landscape of Estrogen receptor-positive breast Cancer Evolution. Cancer Discov. 2024;14:1612–30.
Slaymaker IM, Gao L, Zetsche B, Scott DA, Yan WX, Zhang F. Rationally engineered Cas9 nucleases with improved specificity. Science. 2016;351:84–8.
Chen JS, Dagdas YS, Kleinstiver BP, Welch MM, Sousa AA, Harrington LB, et al. Enhanced proofreading governs CRISPR-Cas9 targeting accuracy. Nature. 2017;550:407–10.
Kleinstiver BP, Pattanayak V, Prew MS, Tsai SQ, Nguyen NT, Zheng Z, et al. High-fidelity CRISPR-Cas9 nucleases with no detectable genome-wide off-target effects. Nature. 2016;529:490–5.
Park J, Yoon J, Kwon D, Han MJ, Choi S, Park S, et al. Enhanced genome editing efficiency of CRISPR PLUS: Cas9 chimeric fusion proteins. Sci Rep. 2021;11:16199.
Wang L, Han H. Strategies for improving the genome-editing efficiency of class 2 CRISPR/Cas system. Heliyon. 2024;10:e38588.
Lahr WS, Sipe CJ, Skeate JG, Webber BR, Moriarity BS. CRISPR-Cas9 base editors and their current role in human therapeutics. Cytotherapy. 2023;25:270–6.
Anzalone AV, Randolph PB, Davis JR, Sousa AA, Koblan LW, Levy JM, et al. Search-and-replace genome editing without double-strand breaks or donor DNA. Nature. 2019;576:149–57.
Pacesa M, Pelea O, Jinek M. Past, present, and future of CRISPR genome editing technologies. Cell. 2024;187:1076–100.
Zeng H, Daniel TC, Lingineni A, Chee K, Talloo K, Gao X. Recent advances in prime editing technologies and their promises for therapeutic applications. Curr Opin Biotechnol. 2024;86:103071.
Tsai SQ, Zheng Z, Nguyen NT, Liebers M, Topkar VV, Thapar V, et al. GUIDE-seq enables genome-wide profiling of off-target cleavage by CRISPR-Cas nucleases. Nat Biotechnol. 2015;33:187–97.
Kim D, Bae S, Park J, Kim E, Kim S, Yu HR, et al. Digenome-seq: genome-wide profiling of CRISPR-Cas9 off-target effects in human cells. Nat Methods. 2015;12:237–43.
Lazzarotto CR, Malinin NL, Li Y, Zhang R, Yang Y, Lee G, et al. CHANGE-seq reveals genetic and epigenetic effects on CRISPR-Cas9 genome-wide activity. Nat Biotechnol. 2020;38:1317–27.
Lazzarotto CR, Nguyen NT, Tang X, Malagon-Lopez J, Guo JA, Aryee MJ, et al. Defining CRISPR-Cas9 genome-wide nuclease activities with CIRCLE-seq. Nat Protoc. 2018;13:2615–42.
Özden F, Minary P. Learning to quantify uncertainty in off-target activity for CRISPR guide RNAs. Nucleic Acids Res. 2024;52:e87.
Mehta A, Merkel OM. Immunogenicity of Cas9 protein. J Pharm Sci. 2020;109:62–7.
Lee JK, Jeong E, Lee J, Jung M, Shin E, Kim YH, et al. Directed evolution of CRISPR-Cas9 to increase its specificity. Nat Commun. 2018;9:3048.
Li J, Wu P, Cao Z, Huang G, Lu Z, Yan J, et al. Machine learning-based prediction models to guide the selection of Cas9 variants for efficient gene editing. Cell Rep. 2024;43:113765.
Harrington LB, Paez-Espino D, Staahl BT, Chen JS, Ma E, Kyrpides NC, et al. A thermostable Cas9 with increased lifetime in human plasma. Nat Commun. 2017;8:1424.
Kim S, Kim D, Cho SW, Kim J, Kim JS. Highly efficient RNA-guided genome editing in human cells via delivery of purified Cas9 ribonucleoproteins. Genome Res. 2014;24:1012–9.
Liu C, Zhang L, Liu H, Cheng K. Delivery strategies of the CRISPR-Cas9 gene-editing system for therapeutic applications. J Control Release. 2017;266:17–26.
Huang Z, Nair M. A CRISPR/Cas9 guidance RNA screen platform for HIV provirus disruption and HIV/AIDS gene therapy in astrocytes. Sci Rep. 2017;7:5955.
Sakurai T, Watanabe S, Kamiyoshi A, Sato M, Shindo T. A single blastocyst assay optimized for detecting CRISPR/Cas9 system-induced indel mutations in mice. BMC Biotechnol. 2014;14:69.
Ramos PD, Almeida MS, Olsson IAS. What do people think about genetic engineering? A systematic review of questionnaire surveys before and after the introduction of CRISPR. Front Genome Ed. 2023;5:1284547.
Sinclair F, Begum AA, Dai CC, Toth I, Moyle PM. Recent advances in the delivery and applications of nonviral CRISPR/Cas9 gene editing. Drug Deliv Transl Res. 2023;13:1500–19.
US National Library of Medicine. http://www.clinicaltrials.gov (2024). Accessed 6 Sept 2024.
Zetsche B, Gootenberg JS, Abudayyeh OO, Slaymaker IM, Makarova KS, Essletzbichler P et al. (2015). Cpf1 is a single RNA-guided endonuclease of a class 2 CRISPR-Cas system. Cell. 2015;163:759–771.
Li S-Y, Cheng Q-X, Liu J-K, Nie X-Q, Zhao G-P, Wang J. CRISPR-Cas12a has both cis- and trans-cleavage activities on single-stranded DNA. Cell Res. 2018;28:491–3.
Li P, Zhang L, Li Z, Xu C, Du X, Wu S. Cas12a mediates efficient and precise endogenous gene tagging via MITI: microhomology-dependent targeted integrations. Cell Mol Life Sci. 2020;77:3875–84.
Guo LY, Bian J, Davis AE, Liu P, Kempton HR, Zhang X, et al. Multiplexed genome regulation in vivo with hyper-efficient Cas12a. Nat Cell Biol. 2022;24:590–600.
Srivastava S, Upadhyay DJ, Srivastava A. Next-Generation Molecular Diagnostics Development by CRISPR/Cas Tool: Rapid Detection and Surveillance of viral Disease outbreaks. Front Mol Biosci. 2020;7:582499.
Abudayyeh OO, Gootenberg JS, Essletzbichler P, Han S, Joung J, Belanto JJ, et al. RNA targeting with CRISPR–Cas13. Nature. 2017;550:280–4.
Zhang Y, Li S, Li R, Qiu X, Fan T, Wang B, et al. Advances in application of CRISPR-Cas13a system. Front Cell Infect Microbiol. 2024;14:1291557.
Huang Z, Fang J, Zhou M, Gong Z, Xiang T. CRISPR-Cas13: a new technology for the rapid detection of pathogenic microorganisms. Front Microbiol. 2022;13:1011399.
Hillary VE, Ceasar SA. A review on the mechanism and applications of CRISPR/Cas9/Cas12/Cas13/Cas14 proteins utilized for Genome Engineering. Mol Biotechnol. 2023;65:311–25.
Wang M, Chen M, Wu X, Huang X, Yu B. CRISPR applications in cancer diagnosis and treatment. Cell Mol Biol Lett. 2023;28:73.
Pandya K, Jagani D, Singh N. CRISPR-Cas systems: programmable nuclease revolutionizing the molecular diagnosis. Mol Biotechnol. 2023 Jul;19. https://doi.org/10.1007/s12033-023-00819-7.
Yoon AR, Jung BK, Choi E, Chung E, Hong J, Kim JS, et al. CRISPR-Cas12a with an oAd induces precise and Cancer-specific genomic reprogramming of EGFR and efficient Tumor regression. Mol Ther. 2020;28:2286–96.
Choi E, Hwang HY, Kwon E, Kim D, Koo T. Expanded targeting scope of LbCas12a variants allows editing of multiple oncogenic mutations. Mol Ther Nucleic Acids. 2022;30:131–42.
Hu T, Ke X, Li W, Lin Y, Liang A, Ou Y, et al. CRISPR/Cas12a-Enabled Multiplex Biosensing Strategy Via an affordable and visual Nylon membrane readout. Adv Sci (Weinh). 2023;10:e2204689.
Kruglova N, Shepelev M. Increasing gene editing efficiency via CRISPR/Cas9- or Cas12a-Mediated Knock-In in primary human T cells. Biomedicines. 2024;12:119.
Palaz F, Ozsoz M, Zarrinpar A, Sahin I. CRISPR in targeted therapy and Adoptive T Cell Immunotherapy for Hepatocellular Carcinoma. J Hepatocell Carcinoma. 2024;11:975–95.
Zhou J, Chen P, Wang H, Liu H, Li Y, Zhang Y, et al. Cas12a variants designed for lower genome-wide off-target effect through stringent PAM recognition. Mol Ther. 2022;30:244–55.
Ryan CJ, Mehta I, Kebabci N, Adams DJ. Targeting synthetic lethal paralogs in cancer. Trends Cancer. 2023;9:397–409.
Gralewska P, Gajek A, Marczak A, Rogalska A. Participation of the ATR/CHK1 pathway in replicative stress targeted therapy of high-grade ovarian cancer. J Hematol Oncol. 2020;13:39.
Parrish PCR, Thomas JD, Gabel AM, Kamlapurkar S, Bradley RK, Berger AH. Discovery of synthetic lethal and tumor suppressor paralog pairs in the human genome. Cell Rep. 2021;36:109597.
Kohabir KAV, Nooi LO, Brink A, Brakenhoff RH, Sistermans EA, Wolthuis RMF. In Vitro CRISPR-Cas12a-Based detection of Cancer-Associated TP53 hotspot mutations beyond the crRNA seed region. CRISPR J. 2023;6:127–39.
Hao L, Zhao RT, Welch NL, Tan EKW, Zhong Q, Harzallah NS, et al. CRISPR-Cas-amplified urinary biomarkers for multiplexed and portable cancer diagnostics. Nat Nanotechnol. 2023;18:798–807.
Zhou H, Tsou JH, Leng Q, Jiang F. Sensitive detection of KRAS mutations by clustered regularly interspaced short palindromic repeats. Diagnostics (Basel). 2021;11:125.
Yang M, Wei H, Wang Y, Deng J, Tang Y, Zhou L, et al. Targeted disruption of V600E-Mutant BRAF gene by CRISPR-Cpf1. Mol Ther Nucleic Acids. 2017;8:450–8.
Sha L, Cao Y, Wang L, Qin Y, Zhu S, Zhao J, et al. An electrochemical biosensor based on mild reduction-activated CRISPR/Cas12a system for sensitive detection of circulating tumor cells. Biosens Bioelectron. 2024;262:116550.
Tsou JH, Leng Q, Jiang F. A CRISPR test for detection of circulating nuclei acids. Transl Oncol. 2019;12:1566–73.
Li SY, Cheng QX, Wang JM, Li XY, Zhang ZL, Gao S, et al. CRISPR-Cas12a-assisted nucleic acid detection. Cell Discov. 2018;4:20.
Antropov DN, Stepanov GA. Molecular mechanisms underlying CRISPR/Cas-Based assays for nucleic acid detection. Curr Issues Mol Biol. 2023;45:649–62.
Montagud-Martínez R, Márquez-Costa R, Heras-Hernández M, Dolcemascolo R, Rodrigo G. On the ever-growing functional versatility of the CRISPR-Cas13 system. Microb Biotechnol. 2024;17:e14418.
Dong Y, Zhang B, Wei Y, Murashev A, Wang S, Wu Y, et al. Development of Cas13a-based therapy for cancer treatment. Mol Biol Rep. 2024;51:94.
Gao J, Luo T, Lin N, Zhang S, Wang J. A New Tool for CRISPR-Cas13a-Based Cancer Gene Therapy. Mol Ther Oncolytics. 2020;19:79–92.
Zhao X, Liu L, Lang J, Cheng K, Wang Y, Li X, et al. A CRISPR-Cas13a system for efficient and specific therapeutic targeting of mutant KRAS for pancreatic cancer treatment. Cancer Lett. 2018;431:171–81.
Xu D, Cai Y, Tang L, Han X, Gao F, Cao H, et al. A CRISPR/Cas13-based approach demonstrates biological relevance of vlinc class of long non-coding RNAs in anticancer drug response. Sci Rep. 2020;10:1794.
Zhang Z, Chen J, Zhu Z, Zhu Z, Liao X, Wu J, et al. CRISPR-Cas13-Mediated knockdown of lncRNA-GACAT3 inhibited cell proliferation and motility, and Induced apoptosis by increasing p21, Bax, and E-Cadherin expression in bladder Cancer. Front Mol Biosci. 2021;7:627774.
Spangler JR, Leski TA, Schultzhaus Z, Wang Z, Stenger DA. Large scale screening of CRISPR guide RNAs using an optimized high throughput robotics system. Sci Rep. 2022;12:13953.
Wang L, Bitar M, Lu X, Jacquelin S, Nair S, Sivakumaran H, et al. CRISPR-Cas13d screens identify KILR, a breast cancer risk-associated lncRNA that regulates DNA replication and repair. Mol Cancer. 2024;23:101.
Kar A, Agarwal S, Singh A, Bajaj A, Dasgupta U. Insights into molecular mechanisms of chemotherapy resistance in cancer. Transl Oncol. 2024;42:101901.
Gootenberg JS, Abudayyeh OO, Lee JW, Essletzbichler P, Dy AJ, Joung J, et al. Nucleic acid detection with CRISPR-Cas13a/C2c2. Science. 2017;356:438–42.
Palaz F, Kalkan AK, Can Ö, Demir AN, Tozluyurt A, Özcan A, et al. CRISPR-Cas13 System as a Promising and Versatile Tool for Cancer diagnosis, therapy, and Research. ACS Synth Biol. 2021;10:1245–67.
Ackerman CM, Myhrvold C, Thakku SG, Freije CA, Metsky HC, Yang DK, et al. Massively multiplexed nucleic acid detection with Cas13. Nature. 2020;582:277–82.
Stefanoudakis D, Kathuria-Prakash N, Sun AW, Abel M, Drolen CE, Ashbaugh C, et al. The potential revolution of Cancer Treatment with CRISPR Technology. Cancers (Basel). 2023;15:1813.
Buchanan G, Vichinsky E, Krishnamurti L, Shenoy S. Severe sickle cell disease–pathophysiology and therapy. Biol Blood Marrow Transpl. 2010;16:S64–7.
El-Beshlawy A, Dewedar H, Hindawi S, Alkindi S, Tantawy AA, Yassin MA, et al. Management of transfusion-dependent β-thalassemia (TDT): Expert insights and practical overview from the Middle East. Blood Rev. 2024;63:101138.
Vyawahare H, Shinde P. Age-related Macular Degeneration: Epidemiology, Pathophysiology, diagnosis, and treatment. Cureus. 2022;14:e29583.
Uddin F, Rudin CM, Sen T. CRISPR Gene Therapy: applications, limitations, and implications for the future. Front Oncol. 2020;10:1387.
Lino CA, Harper JC, Carney JP, Timlin JA. Delivering CRISPR: a review of the challenges and approaches. Drug Deliv. 2018;25:1234–57.
Pineda M, Lear A, Collins JP, Kiani S. Safe CRISPR: challenges and possible solutions. Trends Biotechnol. 2019;37:389–401.
Ewaisha R, Anderson KS. Immunogenicity of CRISPR therapeutics-critical considerations for clinical translation. Front Bioeng Biotechnol. 2023;11:1138596.
Canver MC, Joung JK, Pinello L. Impact of genetic variation on CRISPR-Cas Targeting. CRISPR J. 2018;1:159–70.
Scott DA, Zhang F. Implications of human genetic variation in CRISPR-based therapeutic genome editing. Nat Med. 2017;23:1095–101.
Acknowledgements
Not applicable.
Funding
This work was supported by: AIRC, IG 2019 - ID. 23264 project – P.I. Emma Di Carlo; European Union – NextGenerationEU, Program “MUR-Fondo Promozione e Sviluppo —DM 737/2021”, acronym of the project “TAILOR-30”, P.I. Emma Di Carlo. European Union – NextGenerationEU, Ministero della Salute, PNRR Program, Project “From inflammatory bowel disease to colon cancer: involvement of innate lymphocytes in early pathogenic mechanisms” – ID. PNRR-MAD-2022-12375909, Head of Local Operative Unit - Emma Di Carlo. The funders did not play a role in the design of the study; the collection, analysis, and interpretation of the data; the writing of the manuscript; and the decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
E.D.C.: Writing – original draft, Writing – review & editing. C.S.: Data curation, Writing – review & editing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Di Carlo, E., Sorrentino, C. State of the art CRISPR-based strategies for cancer diagnostics and treatment. Biomark Res 12, 156 (2024). https://doi.org/10.1186/s40364-024-00701-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1186/s40364-024-00701-x