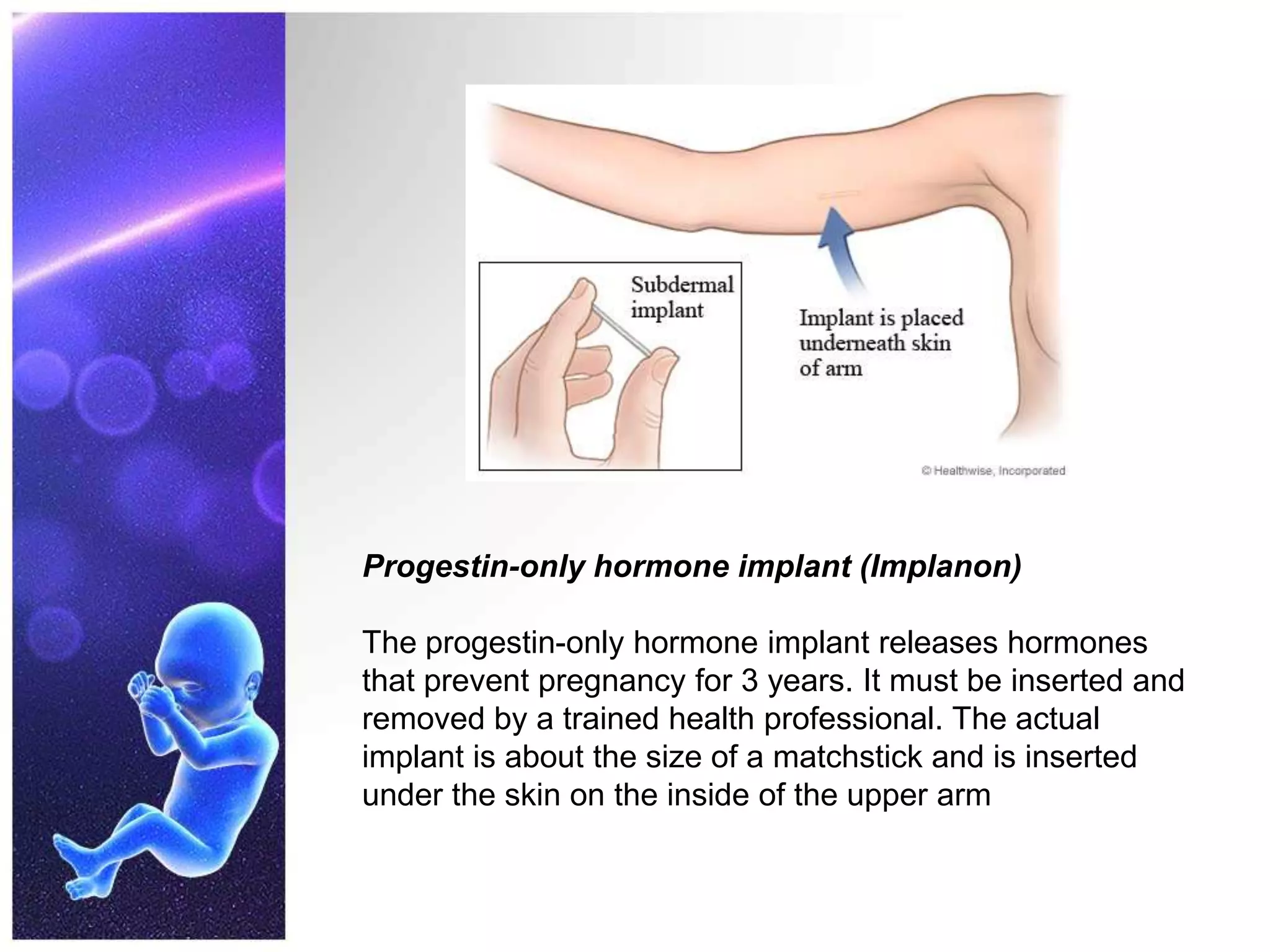
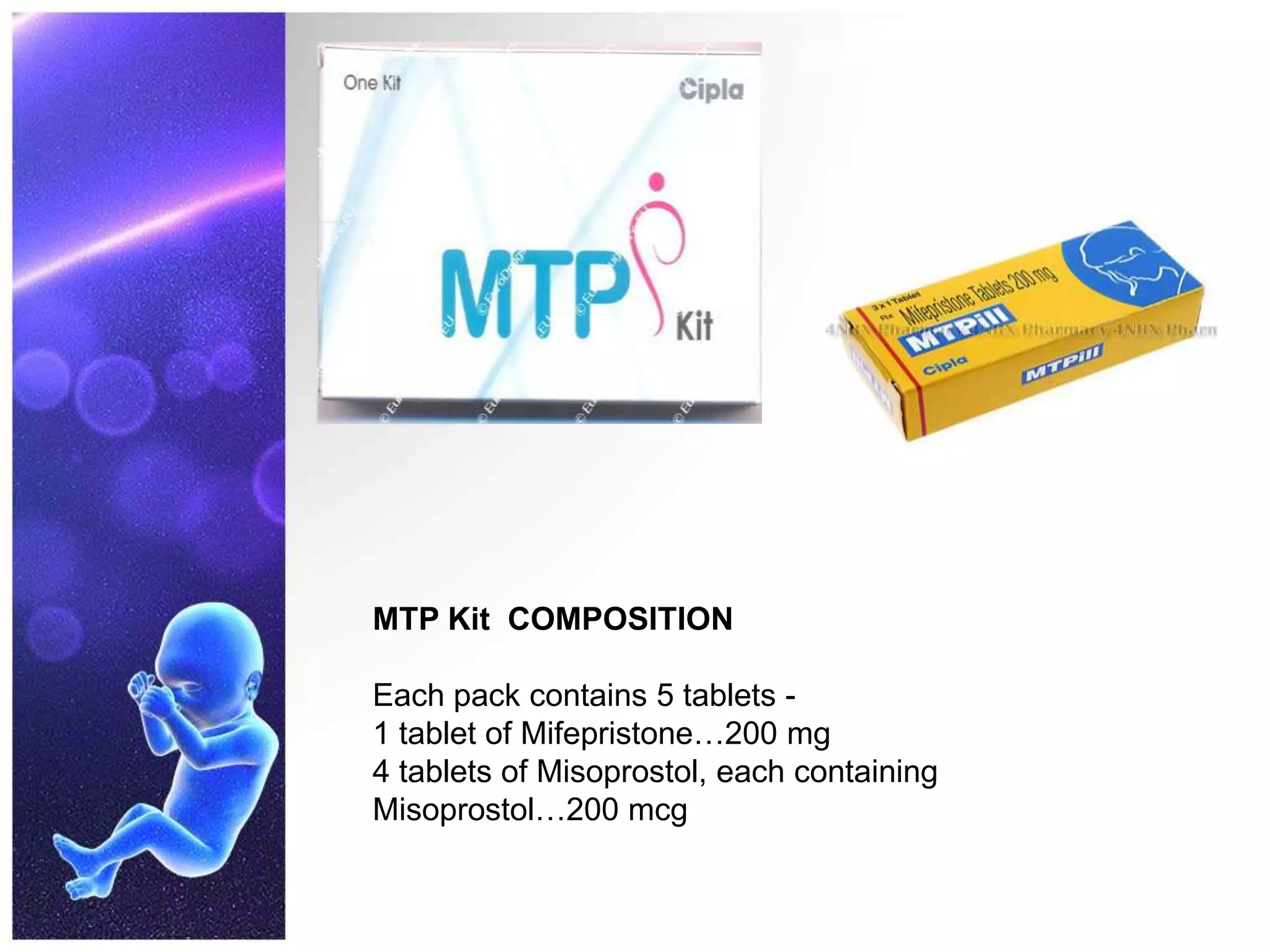
Progesterone is a hormone that prepares the uterus for pregnancy and maintains pregnancy. It is produced naturally by the ovaries and placenta during pregnancy. Synthetic progestins are also used as contraceptives and for hormone replacement therapy. Progestins work by converting the estrogen-primed endometrium to a secretory state and maintaining it to support pregnancy. They also have other effects throughout the body. Mifepristone is a progesterone antagonist that is used to terminate early pregnancies by blocking the effects of progesterone and causing abortion.
![NATURAL PROGESTIN
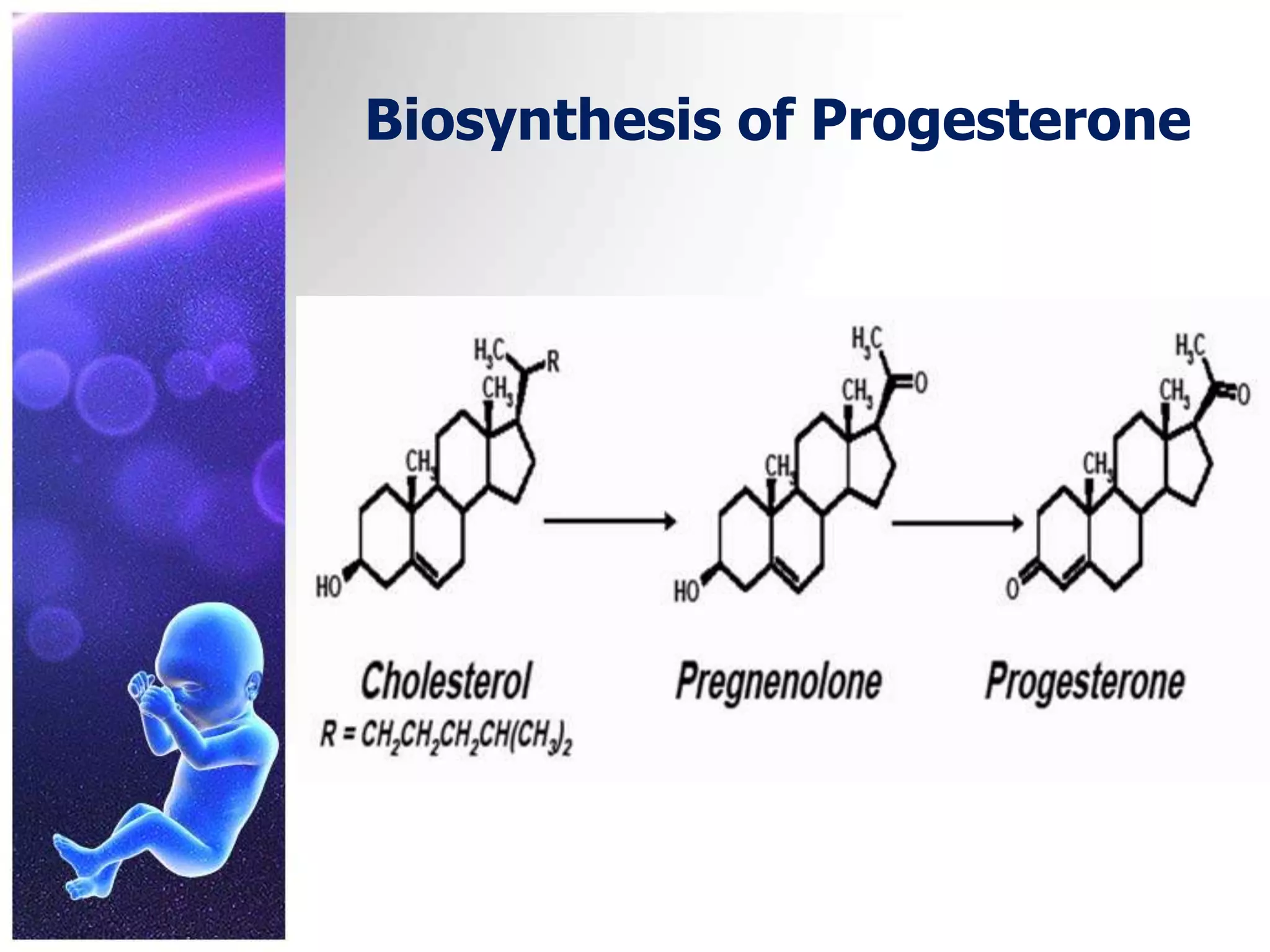
PROGESTERONE (21 CARBON STEROID) is derived from
cholesterol
It was first isolated in 1929
It is secreted by corpusluteum (10-20mg/day) in later half of
menstrual cycle under influence of LH. If ovum gets fertilized
and implants-the blastocyst immediately starts producing
chorionic gonadotropin which is absorbed and sustains the
corpus luteum in early pregnancy. Secretion of progesterone
starts from placenta from 2nd trimester till term
Males also produce 1-5mg progesterone per day from adrenals
and testes
[BUT ROLE IN MALES IS NOT KNOWN]](https://image.slidesharecdn.com/nikilsam-130530105649-phpapp01/75/PROGETINS-3-2048.jpg)