The document discusses autism spectrum disorders including communication disorders, socialization problems, and various conditions on the autism spectrum such as Asperger's syndrome and childhood disintegrative disorder. It notes that autism is characterized by impairments in social interaction and communication as well as restricted and repetitive behaviors. Early intervention is important and can address deficits in communication, social skills, academics and other areas. Treatment is tailored to the individual needs of the child and may involve educational or medical interventions.
Autism Spectrum, SocializationProblems, and Communication Disorders Elyssa Baker Courtney Reinhold Elizabeth Staab Amanda Woloshin
2.
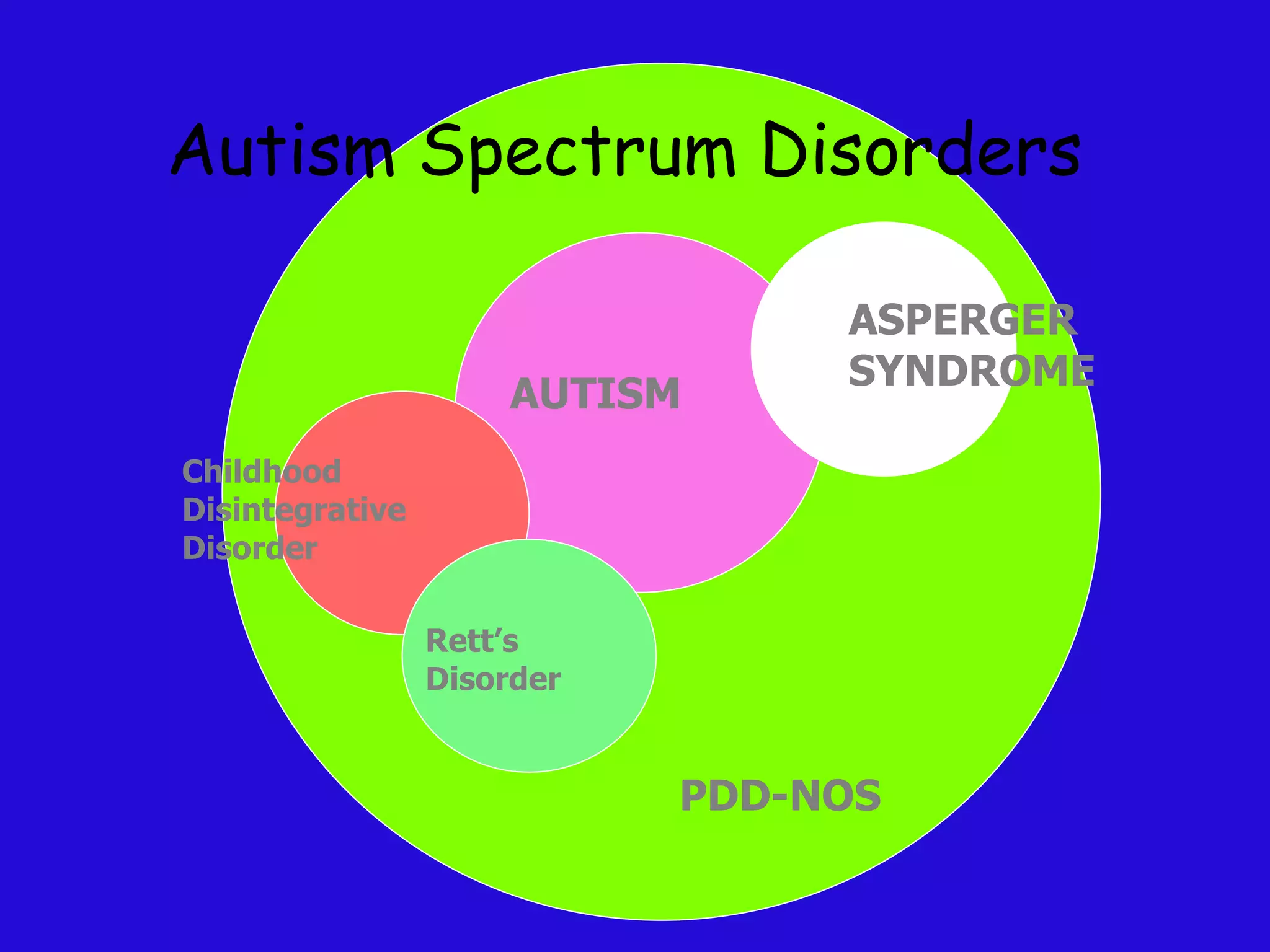
Introduction to AutismSpectrum Disorders Includes: Autism, Aspergers Syndrome, Childhood Disintegrative Disorder, Rett’s Syndrome, and PDD-NOS Disorders are distinguished from each other based on Age of onset Presence of language or cognitive delay Presence of co-morbid factors Specific neurological features
3.
Communication Disorders andSocialization Problems Communication disorder- condition that partially or totally prevents human communication. The defect can be in producing, receiving or understanding the communication. Socialization problem- an inability to perform social skills other than language. (ex. Eye contact, respond appropriately to others, initiate interactions) Kauffman, 2005
4.
Pervasive Developmental Disorder(PDD) Distortion of or lag in all or most levels of development Includes Autism, Rett's disorder, childhood disintegrative disorder, Aspergers, PDD-NOZ
5.
Pervasive Developmental Disorder-NotOtherwise Specified (PDD-NOS) Pervasive delay in development that does not fit into any of the other diagnostic categories Doesn’t fit classification of other PDD disorders, placed here
6.
Childhood Disintegrative Disorder(CDD) Rare condition characterized by late onset (greater than 3 years of age) of developmental delays in 3 areas Language Social Function Motor Skills Similar to Autism, but an apparent period of fairly normal development is noted before regression in skills Children already experience some delay, but delay is not always obvious in young children Kauffman, 2005/wikipedia.com
7.
Rett’s Syndrome Normaldevelopment for 5 months to 4 years, then regression and mental retardation Similar to Autism, especially behavior characteristics X-linked dominant: affecting most exclusively girls, mutation Affects 1/12,500 girls by the age of 12 Girls are very prone to gastrointestinal disorders and about 30% have seizures Typically have no verbal skills, and about 50% of females are not ambulatory Kauffman, 2005/Wikipedia.com
Autism A PervasiveDevelopment Disorder Onset before age of 3 Qualitative impairment of social interaction and communication Restricted, repetitive, stereotyped patterns of behavior, interests, and activities
10.
Symptoms of AutismTRIAD OF IMPAIRMENTS Communication In young children, language delay is a strong indicator of Autism (RISK FACTOR) Social Reciprocity Restricted Interests and Repetitive Behaviors
Prevalence 1 in150 children is diagnosed with autism 1 in 94 boys is on the autism spectrum 67 children are diagnosed per day http://www.autismspeaks.org/whatisit/facts.php
13.
Facts Autism coststhe nation over $90 billion per year, a figure expected to double in the next decade Boys are four times more likely than girls to have autism Autism is the fastest-growing serious developmental disability in the U.S. More children will be diagnosed with autism this year than with AIDS, diabetes & cancer combined http://www.autismspeaks.org/whatisit/facts.php
14.
Etiology There isno real cause of autism. Recent studies suggest a strong genetic basis for autism -- up to 20 sets of genes may play a part in its development. Studies are also looking at possible environment origins and triggers. Movie Clip http://www.youtube.com/watch?v=u4uGWiQgRYs http://www.autismspeaks.org/whatisit/faq.php
15.
Assessment Most childrenare diagnosed by observation. http://www.youtube.com/watch?v=oE9zN1OSKdE
16.
IDEA/EBD Qualifications IDEAdefines autism as “a developmental disability that primarily results in significant deficits in verbal and non-verbal communication and social interactions, generally evidenced before the age of 3 years and adversely affects the child’s educational performance.” (Dowdy, Patton, Polloway, and Smith, 2006)
17.
IDEA/EBD Qualifications (cont.)Fits under IDEA if… Adversely effects the student’s educational performance. An inability to build or maintain satisfactory interpersonal relationships with peers and teachers. Inappropriate types of behavior of feelings under normal circumstances (Kauffman, 2005)
18.
Comorbidity Issues anxietyand depression ADHD mental retardation a behavior disorder problems with hearing odd and eccentric behavior (Autism Society of America, 2000)
19.
Prevention Strategies Thereare two types of prevention according to Kauffman: Primary -involves physiological prevention strategies that include genetic counseling and prenatal care 2. Secondary -consists of early identification and intervention -educational programs play an important role in secondary prevention (Kauffman, 2005)
20.
Intervention Importance ofintensive early intervention for young children across the autism spectrum These children share a common diagnostic label, each has own individual needs. Intervention should address the core deficits that the ASD share communication social problems sensory problems academic difficulties (Autism Society of America, 2000)
21.
Intervention (cont.) Foreffective intervention, parents and professionals should consider the following: 1. A curriculum which addresses deficit areas Deficit areas include: Inability to attend to relevant aspects of the environment, to shift attention, and to imitate language and the actions of others; 2. Difficulty in social interactions;
22.
Intervention (cont.) 3.Difficulty with language comprehension and use, and functional communication 4. Programs that focus on routines, schedules, and predictability 5. Coordinated transitions between early intervention/preschool programs, and kindergarten environments
23.
Intervention (cont.) 6.Family involvement, including coordination between home and involved professionals, an in-home training component, and family training and support (Autism Society of America, 2000)
24.
Treatment Options Thereis no one symptom or behavior that identifies individuals with ASD which leads to having no single treatment that will be effective for all people on the spectrum Treatment must begin as early as possible and be tailored to the child's unique strengths, weaknesses and needs. Treatments may be obtained through either the medical or educational community, depending on the nature of the treatment
25.
Medical Treatment Thereare no drugs, vitamins or special diets that can correct underlying neurological problems associated with autism Changes to diet and the addition of certain vitamins or minerals may also help with behavioral issues that occur with Autism Stimulants, such as Ritalin, Adderall and Dexedrine, used to treat hyperactivity in children with ADHD have also been prescribed for children with ASD due to the behavior problems that are common in children with ADHD (Autism Society of America, 2000)
Aspergers Syndrome “Children with Asperger syndrome do not show clinically significant general delay in language, nor do they show significant delay in cognitive development or the development of age appropriate self-help skills or adaptive behavior. Thus, although they have significant problems in socialization and manifest some of the peculiarly obsessive or repetitive behaviors of children with autism, their language and cognitive development are much more normal than is typical for autism.” (Kauffman, 2005)
28.
Aspergers Syndrome Characteristics Marked impairment in the use of multiple nonverbal behaviors such as eye-to-eye gaze, facial expression, body postures, and gestures to regulate social interaction Failure to develop peer relationships appropriate to developmental level A lack of spontaneous seeking to share enjoyment, interests, or achievements with other people (e.g., by a lack of showing, bringing, or pointing out objects of interest to other people) Lack of social or emotional reciprocity http://www.autism-society.org/site/PageServer?pagename=about_whatis_asperger
29.
Intervention and TreatmentAspergers syndrome can be treated and can take the same intervention methods as a person with autism People with Aspergers syndrome need special attention with socialization problems when intervening
30.
ASD Spectrum PrognosisBecause of such a wide spectrum, there are not any certain characteristics that can be applied to each person with autism No two children will have the same outcome later in life living with autism
31.
Case Study Charlie’sparents noted something different about their child when he was about 2 years old. Up until that time he had developed perfectly. He walked at 13 months, started babbling at about 15 months, and loved to play with adults and other children. Then things began to change. His babbling stopped, he developed sort of a blank stare, his early success at toilet training seemed to be reversed, and he stopped paying attention to other children and adults. When he was about 3 years old, his parents took him to the state children’s hospital, and the diagnosis was autism. What a shock! Charlie was placed in a preschool program and has been in special education services ever since. Now at the age of 7 he is enjoying being in a regular second grade classroom. In his kindergarten and first grade experience he was placed in a self-contained special education classroom. During these two years Charlie seemed to regress. He actually started picking up some of the other children’s stereotypical, self-stimulating behaviors. His parents convinced the school to give Charlie a try in the regular second grade, with some special education support. Now, in December, Charlie seems to be doing very well. While he has very little oral language, he seems to enjoy being with his nondisabled peers and is able to do most of the academic work with the assistance of a paraprofessional. (Dowdy, Patton, Polloway, and Smith, 2006)
32.
Case Study QuestionsWhere on the ASD would you place Charlie and why? Is there a preferred placement for children with autism? What kinds of supports should be available for Charlie to facilitate his success in the regular classroom? Is a child ever ready for inclusion, or does the school have to make the placement decision and provide the necessary supports to make it work? As a parent where would you want Charlie placed, and what could you do to ensure Charlie is receiving supports at home as well as school?















![Autism[1]_PP](https://cdn.slidesharecdn.com/ss_thumbnails/10451173-111203205113-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)






































































